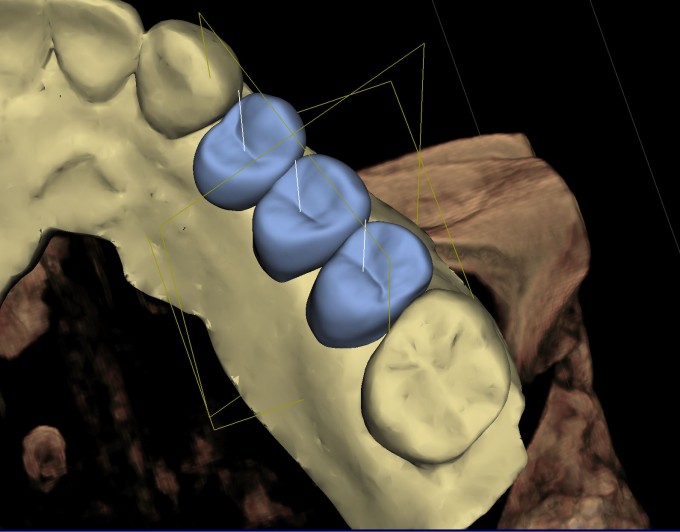
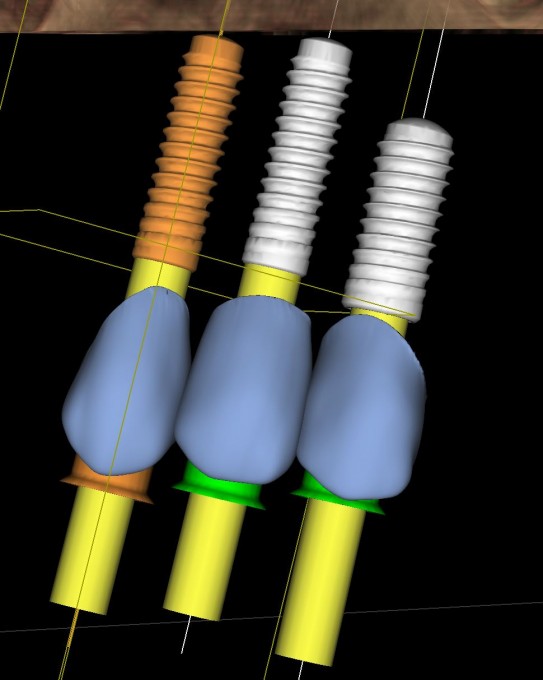
3 Teeth/Implants Vs. 2 Teeth/Implants

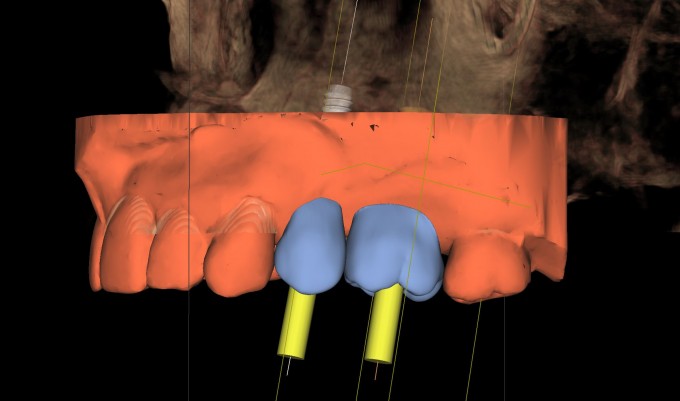
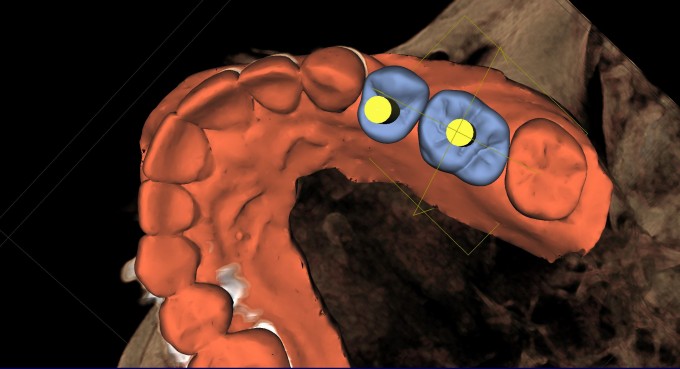
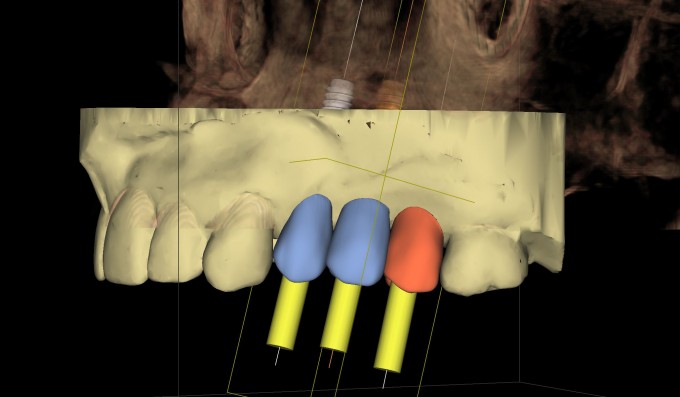
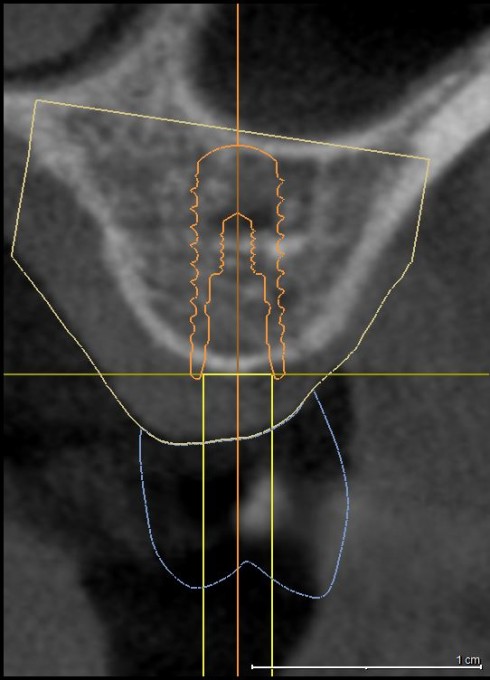
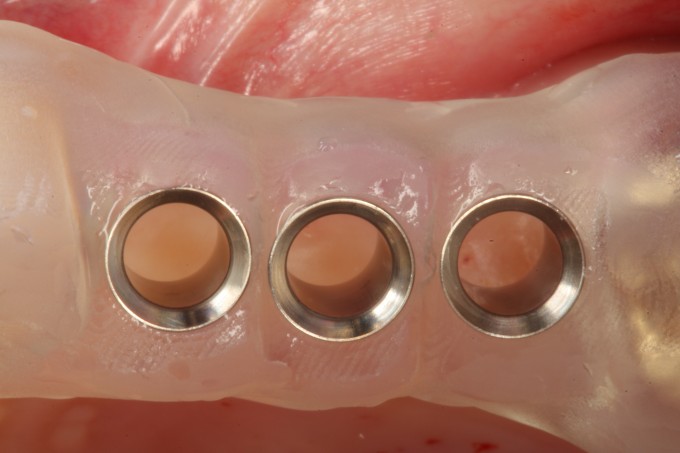
There are situations where the spacing for implant therapy is not ideal one way or the other. With the CEREC-Galileos integration we have the ability to create 2 different plans and decide which one works better.
What do you guys think, 2 or 3?
Farhad

I’d be looking at interimplant bone in the 3 unit case if I were doing the planning- since you’ve done this I assume that dimension is comfortable. I’d also be looking at restorative space in the ability to do multilayer with at least 2 of the units— I’d hate 3 adjacent screw retained, and prefer splitting anyways. Just easier and more flexible with material options. The main downside to me generalizing to the 2 is gingival embrasure space. But other than that (which is big) I’d be thinking 2...not the worst spacing in the world - I’ve seen worse all the time

I personally prefer a screw retained 3 unit bridge on non engaging custom abutments. I find it easier to clean one space with a floss threader and I have an easier time creating a nice ovate Pontic with papilla formation.
I use TruAbutment for custom non engaging abutments with ASC if Necessary. I believe they can also provide a “seated in place abutment model” so you can design and mill the bridge yourself or they will do it for you.


Farhad
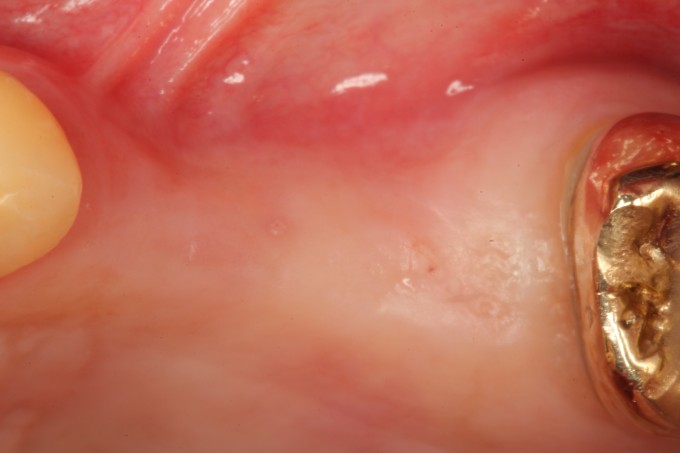
Such an interesting situation where you can still have 3 mm in between implants and 3 crowns
- looking at the contralateral side and the tooth dimension that you have on the right I would consider 2 implants and creating the ideal emergence to minimize gingival embrasures , and the other aspect is to see how the esthetic will be impacted with small bicuspids vs bicuspid and molar
Occlusion can also play a role with
If this was a 4 bicuspid extraction case and how the occlusal contact can be established
Flavio

If three implants aren't a deal breaker because of cost, the 3 premolars/implants might be preferable because of better, more cleansable emergence profiles.

2 units for me in general. Mainly because of cleaning. Getting someone to clean adequately around 2 implants is tough enough.




On 9/23/2018 at 6:21 pm, Josh Fowler said... 2 units for me in general. Mainly because of cleaning. Getting someone to clean adequately around 2 implants is tough enough.
I don't think it is any more difficult to clean around 2 or 3 implants than it is to clean around 2 or 3 teeth. I have had my #14 implant for 20 years. I floss it just as I do the rest of my teeth. No different.
On 9/24/2018 at 12:49 pm, Mark Stockwell said...Nice... and you're a big tease...
Mark
Thanks Mark but I was honestly not teasing. I just did this case this morning so I wanted to see how some great restorative dentists look at this and the answers were all correct. I ultimately ran both options by the patient and her restorative dentist (a CEREC master) and the patient decided to go with 3 implants and 3 teeth because she wanted to prevent food impaction and open embrasures as much as possible. I have almost never seen any food impaction around a premolar implant but most of the molar implants end up with some sort of food impaction. I have 2 premolar implants and one molar implant myself and I am no exception to that. Downside to the 3 implant option is that the restorative treatment will be a little more challenging with regard to the interproximal contacts but her restorative dentist is superb so I am sure he will handle it.
Farhad

Excellent case Farhad. I typically will disk adjacent teeth with molar implants to have long occlusal-apical and buccal-lingual contacts to prevent food impaction.
What do think?
I think that’s a great idea Damen and helps in standard situations more than cases like this with oversized molars or too mesially tilted adjacent teeth.
Farhad

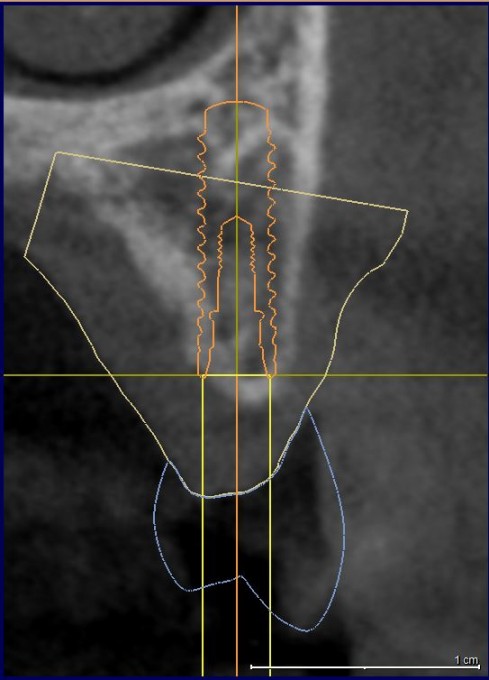
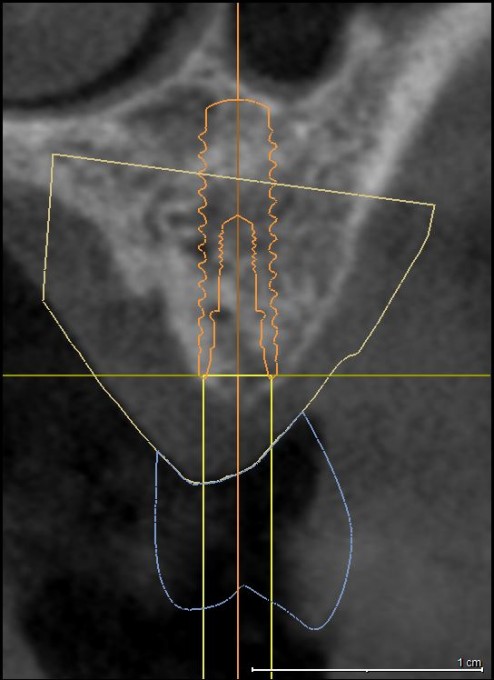
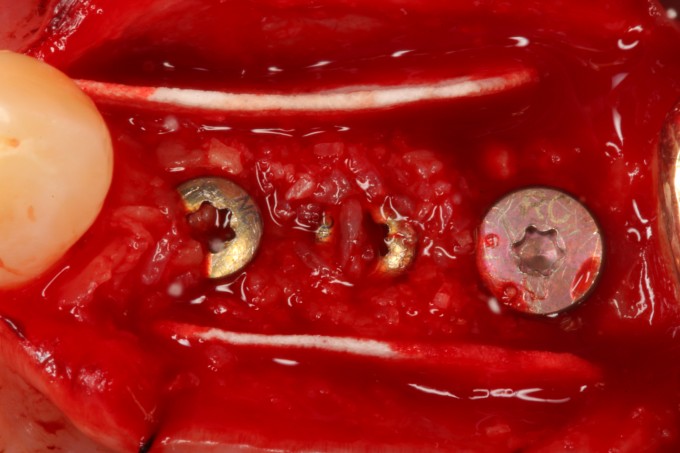
Farhad, I noticed the distal most implant was planned slightly supra crestal, but the implant looks a bit sub crestal in the placement photo. Did you plan it this way to prevent the drills from perforating the sinus during the osteotomy and then you free handed it to depth without the guide as you mentioned in my other post? This might be a great case for Atlantis abutments since minimal thickness will likely be an issue with a TiBase here. Beautiful surgery as usual.
Yes exactly Dan. I did it exactly as we discussed on the other thread. I think this will definitely be an Atlantis case. BTW: This was a 3 SiCat sleeve-in-sleeve digital guide...when the spaces are tight I love the sleeve-in-sleeve option.
Farhad
On 9/24/2018 at 1:14 pm, Farhad Boltchi said...Actually to be honest I just listened to Dr. Chuck.
Farhad
Now THERE is a title of a book....
Mark

Nice case and nice discussion.
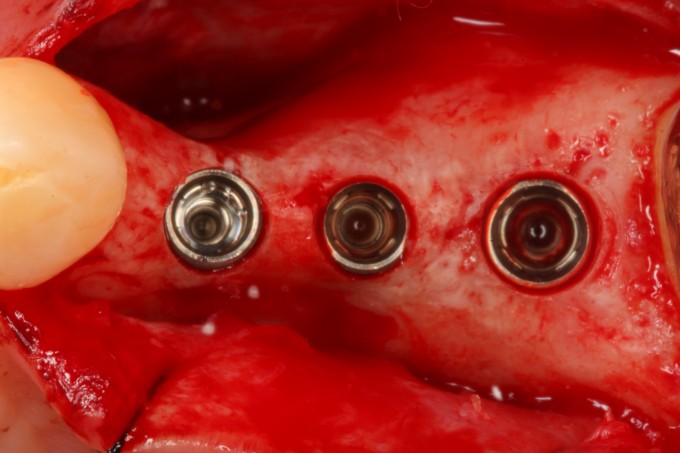
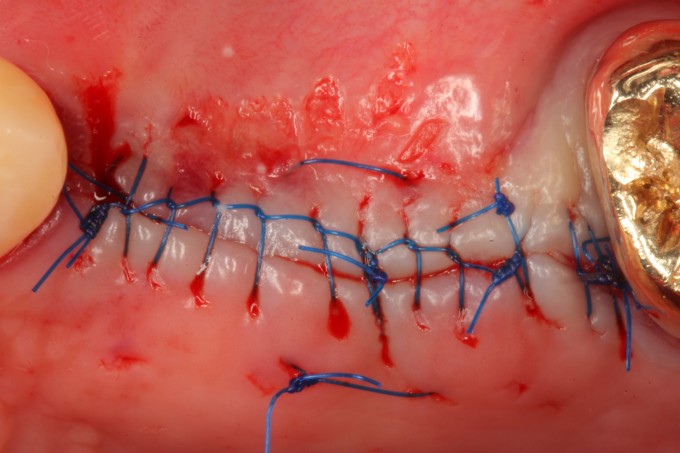
Your sutures are so nice,,,
Now the next question, with 3 you most likely do not need to splint (not knowing the occlusion etc.) With 2 would you have splinted them>?
On 9/24/2018 at 5:36 pm, Robert Lang said...Nice case and nice discussion.
Your sutures are so nice,,,
Now the next question, with 3 you most likely do not need to splint (not knowing the occlusion etc.) With 2 would you have splinted them>?
Either way I would not have splinted. Nowadays I only splint 6mm implants.
Farhad
Beautiful case Farhad. The patient will be super happy with your 3 implant plan and when its fully restored. ![]()

Just checked back on this thread.... beautiful surgery! My favorite thing about it is that instead of just "squeezing in" an implant into a narrow ridge, you grafted to achieve an ideal result.
As for the 2 vs 3 debate, obviously either works fine... especially when executed to this level. I still would do 2 as my preference. Less cost for the patient, more inter-implant bone and soft tissue, and less restorative complexity.
On 9/26/2018 at 2:04 pm, David Sullivan said...Just checked back on this thread.... beautiful surgery! My favorite thing about it is that instead of just "squeezing in" an implant into a narrow ridge, you grafted to achieve an ideal result.
As for the 2 vs 3 debate, obviously either works fine... especially when executed to this level. I still would do 2 as my preference. Less cost for the patient, more inter-implant bone and soft tissue, and less restorative complexity.
David,
Completely agree with all your points. In this case I had 2 guides printed to go either way. At the end it simply came down to the patient wanting to minimize food impaction as much as possible.
Farhad

A colleague of mine has a patient with a similar situation to this case, where you could plan 2 oversized implant crowns or squeeze 3 implant crowns in. He asked me to help him plan it and currently there is maybe 2mm bone at the crest between implants. If we platform switch a 4.7mm implant to a 3.5 platform, instead of a 4.5 platform, does that give us the extra millimeter we are looking for? Should we calculate interimplant bone from platform to platform instead?
On 9/27/2018 at 3:21 pm, Mark Minchow said...A colleague of mine has a patient with a similar situation to this case, where you could plan 2 oversized implant crowns or squeeze 3 implant crowns in. He asked me to help him plan it and currently there is maybe 2mm bone at the crest between implants. If we platform switch a 4.7mm implant to a 3.5 platform, instead of a 4.5 platform, does that give us the extra millimeter we are looking for? Should we calculate interimplant bone from platform to platform instead?
For posterior platform-switched implants 2mm between implants is adequate.
Farhad

This was a cortical min/demin allograft (Maxxeus) mixed with PRF covered by a pericardium membrane (Copi-Os Extend) and then a layer of PRF membrane on top (not pictured). Ordinarily I would have added a second layer of a xenograft but since this was a relatively small defect I didn’t.
Farhad