Leveraging Time with CEREC (ROI)

We all know CEREC is capable of producing great aesthetic results, makes restoring implants easier/faster, and can even mill surgical guides in office. For me, one of my favorite procedures is the same day root canal, build up, and crown. I know the clinical situation doesn’t always allow it, but when it does, I find that CEREC allows me to leverage my time for both the benefit of the patient and myself.
Last week, this patient appointed for an OB resin on tooth #30 and a root canal, build up, crown on tooth #31. The appointment was scheduled for 7 AM and the patient was out before 9. The appointment workflow looks something like this:
- Seat/numb patient (1 septo)
- Capture pre-op images of the opposing arch, BB, and mandibular arch.
- Use the cut tool to remove tooth #31.
- Deliver second carpule of anesthetic (septo)
- Place IsoDry.
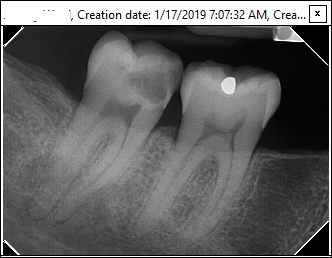
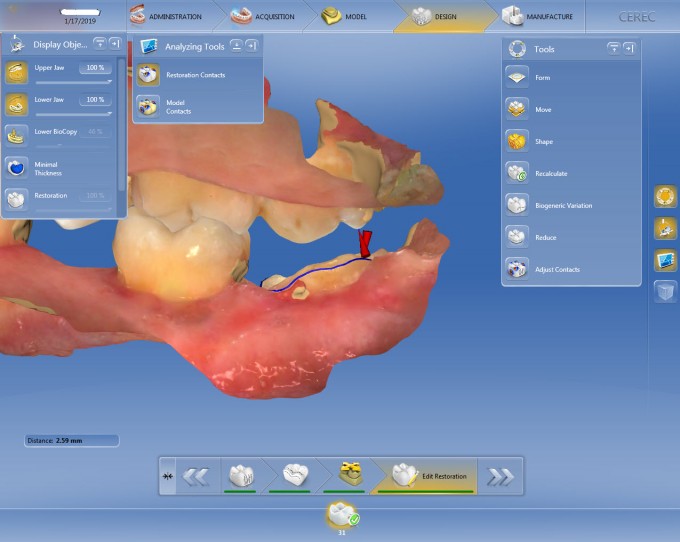
- Prepare #31. I didn’t have to spend much time searching for the canals as the decay already involved in the pulp chamber. Also, reviewing my CBCT prior to treatment let me know exactly how many canals there were. As I know I’m doing a root canal, I don’t have to be timid about my occlusal reduction. As you can see, this is anything but a traditional prep. I would guess my prep took ~10 minutes. I don’t want to image with the pulp chamber opened, so I placed some packable resin and just took a few seconds to smooth it, simulating my core build-up (don't bond this into place).
- Capture CEREC images and pass the AC unit to my second assistant to design, mill, fire the restoration.
- Place rubber dam, remove resin in chamber, start RCT.


The RCT is relatively quick as I had already found my canals. Also, using my CBCT to estimate canal length and an M4 handpiece making getting to length relatively easy. The crown is usually out of the oven when I’m finished and is ready for try-in. I always seat the crown and let the patient see what it looks like to get their approval. After that, it’s prepared for bonding. The IsoDry is placed again in the crown is bonded in place. The resin on #30 can be completed at any time; before CEREC images, after bonding crown, etc.
The power of certain comes into play in that the crown preparation is completed prior to the RCT. If I find that I can’t get the canals dry or I need a second appointment to complete the RCT for whatever reason, I will usually mill an MZ 100 and bond that in the interim.

great work flow Steve. The beauty of cerec is being able to manufacture the crown at the same time as the endo so you are not making the appointment that much longer. One of the best ROI visits for us and Pt only has to be in the office for a single visit. Don't discount how much that means to them. Well done as always sir!

Awesome treatment Steve. Most docs automatically do the rootcanal before the crown prep, but reversing the order as you did makes fantastic use of the milling and oven time. Great service for your patient!

Thanks for sharing this case. This type of appointment has been very powerful for me as well. Patients absolutely love it. I have always enjoyed endo, but this has made it much more efficient and profitable. I heard people talk about how CEREC will make patients say yes, but I under estimated the true value of that, especially for this type of appointment.
I purchased my practice 3 years ago, and the previous dentist did endo. He did nice work, had been here for a long time, and was respected in the community. His patients were use to two appointment root canals as the norm, and then another appointment for crown prep, and another appointment for seating. That is 4 appointments to have a RCT/BU/Crown in most situations. I can now tell these same patients I can do the same thing in about 2 hrs, do it at a very high level of comfort, and with quality results. Its a huge benefit to patients and that makes me happy as a provider.
Thanks for sharing your workflow!
Kyle Dixon

Excellent Steve! Nice workflow, great explanation on efficiency and leveraging time.... shouldn't be lost on even the Cerec geeks what an excellent RCT! ![]()
Mark


On 1/23/2019 at 10:45 am, Jeanie Luong said... Really nice RCT!! What obturation system do you use?
Gutta Core by Sybron Endo

On 1/23/2019 at 1:58 pm, Steven Hernandez said...On 1/23/2019 at 1:27 pm, Armin Giessmann said...Steven, Steven, you forgot #30 resin OB!


On 2/2/2019 at 4:09 am, Armin Giessmann said...On 1/23/2019 at 1:58 pm, Steven Hernandez said...On 1/23/2019 at 1:27 pm, Armin Giessmann said...Steven, Steven, you forgot #30 resin OB!

On 2/2/2019 at 4:09 am, Armin Giessmann said...On 1/23/2019 at 1:58 pm, Steven Hernandez said...On 1/23/2019 at 1:27 pm, Armin Giessmann said...Steven, Steven, you forgot #30 resin OB!
Armin, it’s hard to make the judgement you have without all the info. There is no pre op pic of the decay but the xray shows a massive lesion which prob had little to no underlying support of enamel since all that dentin is now decay. With all that undermined enamel, there is a good chance that a lot of it needed to be removed. The beauty of cerec is we don’t have to prep to hold a temp. We have adhesive dentistry to help us. There is still resistance form on the buccal and lingual. Steve, I personally like to do the same time management steps in cases like this when I can. Thanks for showing the workflow

Steve,
Great work. I love that work flow and I use it whenever there is enough tooth structure apical to the crown margin to hold a rubber dam clamp. The patient isn't in the chair too much longer than if only the crown was being done. One other issue that can rear its ugly head is that, if the patient is insurance driven, an endo, core, and crown could max out the patient in one visit. I have lost track of the number of times since I have been a CEREC dentist that I have done the endo in December and the core and crown in January. Doing the crown prep first makes the endo much easier to complete also. I wish I could use this work flow more than I do. Armin, I am going to go beyond what Dr. Rosenblatt just posted and say that accusing Dr. Hernandez of "radical decapitation " of a tooth when you haven't seen a pre op photograph or radiograph of the case is totally out of line. Knowing Dr. Hernandez as I do, I am quite certain that this molar was totally bombed out and this is a "herodontics" case well executed.
Richard and Charles,
yes, indeed, no photo.
But looking at the X-ray it seems to me at least doubtful that it was absolutely necessary to cut down this tooth on the distal so far.
And supposed it is inevitable to cut the tooth down in the whole distal area then there is an indication to place a post and do a core build-up to get the forces away from just the bonding area and lead them also to the other tooth structures.
And as I said: I do not see why the distal guttapercha is not shortened to root length. This reduces the long-term survival of the tooth and usually creates needless post-operative sensitivities.
This case gave me the impression that the speed and efficiency aspect is sometimes overrated. Sometimes we have cases that require more effort than average and sometimes it pays not really off in the economic way. On the other hand: Sometimes we have cases that are so easy to handle that it pays off better than we deserve.
Charles, I bet you would have solved this case differently.
I think this is a forum where we can discuss objectively and constructively about cases presented. I do not see signs that we have to applaud to everything that is presented or at least remain silent. I have a different understanding of a case discussion.
There were some personal comments on my last comment that I will joyfully ignore.
On 2/2/2019 at 10:06 am, Armin Giessmann said...Richard and Charles,
yes, indeed, no photo.
But looking at the X-ray it seems to me at least doubtful that it was absolutely necessary to cut down this tooth on the distal so far. It is my opinion that this conclusion cannot be reached with certainty without at least a pre-op photograph, radiograph, or better yet, both. In my opinion there is not enough pre-op information for you to be so positive.
And supposed it is inevitable to cut the tooth down in the whole distal area then there is an indication to place a post and do a core build-up to get the forces away from just the bonding area and lead them also to the other tooth structures. I can agree with this point, but I have had decent success building up broken down teeth without a post. I have had some of these de-bond after a few years, the number of years varies, and fiberglass posts, core and crown come out in one piece. Every situation is different.
And as I said: I do not see why the distal guttapercha is not shortened to root length. This reduces the long-term survival of the tooth and usually creates needless post-operative sensitivities. That slight extrusion of gutta percha in the distal canal does not bother me in the slightest. It will not negatively affect the success of this restoration. There are none of us who do endo that exactly nail every root canal filling to the perfect length. A fraction of a millimeter too long and the apical stop can be compromised. I dare say, it has happened to all of us.
This case gave me the impression that the speed and efficiency aspect is sometimes overrated. Sometimes we have cases that require more effort than average and sometimes it pays not really off in the economic way. On the other hand: Sometimes we have cases that are so easy to handle that it pays off better than we deserve. Yes, speed and efficiency can be over rated. Every case is different. Steve was simply making a point for new users.
Charles, I bet you would have solved this case differently. Don't be too sure. Dr. Hernandez is one dentist I will not second guess.
I think this is a forum where we can discuss objectively and constructively about cases presented. I do not see signs that we have to applaud to everything that is presented or at least remain silent. I have a different understanding of a case discussion. I agree. We can discuss objectively, but some of us come across a little too strongly. I am guilty of that. I will add one observation, which has been pointed out to you before. I don't believe that you have posted even one of your own cases. It is difficult to take someone seriously who doesn't back up his words with some "bona fides."
There were some personal comments on my last comment that I will joyfully ignore. Translation: "There is nothing to discuss here. I am right, as always. You and Dr. Rosenblatt are wrong."
I am done here. We need to agree to disagree.
On 2/2/2019 at 3:07 pm, Charles LoGiudice said...On 2/2/2019 at 10:06 am, Armin Giessmann said...Richard and Charles,
yes, indeed, no photo.
But looking at the X-ray it seems to me at least doubtful that it was absolutely necessary to cut down this tooth on the distal so far. It is my opinion that this conclusion cannot be reached with certainty without at least a pre-op photograph, radiograph, or better yet, both. In my opinion there is not enough pre-op information for you to be so positive.
And supposed it is inevitable to cut the tooth down in the whole distal area then there is an indication to place a post and do a core build-up to get the forces away from just the bonding area and lead them also to the other tooth structures. I can agree with this point, but I have had decent success building up broken down teeth without a post. I have had some of these de-bond after a few years, the number of years varies, and fiberglass posts, core and crown come out in one piece. Every situation is different.
And as I said: I do not see why the distal guttapercha is not shortened to root length. This reduces the long-term survival of the tooth and usually creates needless post-operative sensitivities. That slight extrusion of gutta percha in the distal canal does not bother me in the slightest. It will not negatively affect the success of this restoration. There are none of us who do endo that exactly nail every root canal filling to the perfect length. A fraction of a millimeter too long and the apical stop can be compromised. I dare say, it has happened to all of us.
Yes, definitely. It happens to me at least once a week that the apical stop is too long. I see it on the control pic of the root filling. And then I try to correct it. Why should I not try that? Too long is always correctable, too short not.
I do not agree that the length of the guttapercha cannot cause a granuloma.
This case gave me the impression that the speed and efficiency aspect is sometimes overrated. Sometimes we have cases that require more effort than average and sometimes it pays not really off in the economic way. On the other hand: Sometimes we have cases that are so easy to handle that it pays off better than we deserve. Yes, speed and efficiency can be over rated. Every case is different. Steve was simply making a point for new users.
Charles, I bet you would have solved this case differently. Don't be too sure. Dr. Hernandez is one dentist I will not second guess.
I think this is a forum where we can discuss objectively and constructively about cases presented. I do not see signs that we have to applaud to everything that is presented or at least remain silent. I have a different understanding of a case discussion. I agree. We can discuss objectively, but some of us come across a little too strongly. I am guilty of that. I will add one observation, which has been pointed out to you before. I don't believe that you have posted even one of your own cases. It is difficult to take someone seriously who doesn't back up his words with some "bona fides."
Oh yes, I did. You did not notice or do not remember them
There were some personal comments on my last comment that I will joyfully ignore. Translation: "There is nothing to discuss here. I am right, as always. You and Dr. Rosenblatt are wrong."
You got that translation wrong I can very well accept your points of view. But not only you and Richard were commenting.
I am done here. We need to agree to disagree.

It looks like it is sealer expressed which many of the sealers in the market will be absorbed. I. My mouth I would rather have a rct with this immediate post op appearance then one that is too short
I see here sealer pushed over the apex: no problem. Will be resorbed
I see here a guttapercha point pushed over the apex: potential problem.
A too short guttapercha point means that there is room for bacteria: problem.
A too long guttapercha point means that direct irritation of the bone can cause inflammation: problem.
Thanks to all those who took the time to dissect my work. I appreciate the time and constructive criticism.
Know that I am ‘woke’ now and realize I am not worthy to practice Dentistry. I shall quit post haste and find another profession.
It takes guts and conviction to post your work on an open forum such as this. I stopped posting radiographs years ago when I would get beat up by armchair quarterbacks with keyboard muscles who never shared their own work. Keep posting Dr. Hernandez. Your efforts to enhance the CEREC community are most respected.
On 2/3/2019 at 10:24 am, Bob Conte said...It takes guts and conviction to post your work on an open forum such as this. I stopped posting radiographs years ago when I would get beat up by armchair quarterbacks with keyboard muscles who never shared their own work. Keep posting Dr. Hernandez. Your efforts to enhance the CEREC community are most respected.
+1
Great job Steve! The service you provided for your patient in regards to quality and timeliness with this workflow is unmatched no matter what anyone says.

Thanks Steve, this gave me some great insight to my RCT, B/U & Crown scheduling. And I think your result is good. I have been scheduling 3 hours and going the longer route, but this is certainly something I can add to my tool box.
On 2/3/2019 at 10:24 am, Bob Conte said...It takes guts and conviction to post your work on an open forum such as this. I stopped posting radiographs years ago when I would get beat up by armchair quarterbacks with keyboard muscles who never shared their own work. Keep posting Dr. Hernandez. Your efforts to enhance the CEREC community are most respected.
I stepped away for a bit and wow.
It takes allot to post anywhere, time and guts. You open itself up to allot... I have never posted anything that I could not find fault with.
This case was a great demonstration of efficient time management for,digital dentistry. If every case I did looked this good I would be very happy.

Thank you for sharing this case, I have wondered what the workflow is when people do this!
I actually have a question for everyone that does the crown prep first and then endo. I have never seen anyone explain their process for this but once the endo is complete, do you add your build up and stop short so that the crown seats all the way and allow cement to fill that area?
Also, if you are doing a traditional crown prep and the decay is extensive on the mesial, do you etch bond and then build your axial wall where the decay was so that you have your definite axial wall? I would imagine it would be hard to rebuild this exactly for the crown to fit but I would find it difficult to bond in resin before the RCT is done.
On 2/3/2019 at 11:36 pm, Jason Boeskin said...Thank you for sharing this case, I have wondered what the workflow is when people do this!
I actually have a question for everyone that does the crown prep first and then endo. I have never seen anyone explain their process for this but once the endo is complete, do you add your build up and stop short so that the crown seats all the way and allow cement to fill that area? Yes
Also, if you are doing a traditional crown prep and the decay is extensive on the mesial, do you etch bond and then build your axial wall where the decay was so that you have your definite axial wall? I would imagine it would be hard to rebuild this exactly for the crown to fit but I would find it difficult to bond in resin before the RCT is done. I have had success using Vertise Flow for this. It is a self bonding flowable composite. I have been able to control it well enough that I have been able to keep it from covering a canal orfice. I build it up in small increments. It bonds well enough that the irrigant is contained within the pulp chamber. When the endo is finished I complete the core composite as usual.

Interesting series of posts. I’m pretty much a stalker on the site (don’t post much) however having done that type of workflow quite often....the one thing I always comment to my assistant about is : why can’t the software propose my core buildup design. Wouldn’t the composite cement when placed create a cohesive buildup/bond to crown upon cementation? I’ve used the add and shape tool to try but it’s not a real efficient or accurate way of doing things.
A composite core can be milled if desired. Now that we are striving to keep access cavities as small as possible, there are more undercuts in the pulp chambers. My preference is for a separate core composite. I use a dual cure flowable core composite and I get it to flow into the undercuts using a lentulo spiral in the slow speed handpiece.
On 2/4/2019 at 9:49 am, Alan Dechter said... Interesting series of posts. I’m pretty much a stalker on the site (don’t post much) however having done that type of workflow quite often....the one thing I always comment to my assistant about is : why can’t the software propose my core buildup design. Wouldn’t the composite cement when placed create a cohesive buildup/bond to crown upon cementation? I’ve used the add and shape tool to try but it’s not a real efficient or accurate way of doing things.
Alan. I have prepped out for the crown, removed the decay and just filled in the hole with composite and cured it before I started the endo. I than scan that and send it to the mill. You can then open another case, scan the prep in biocopy and then remove the composite you put in there and before you do the endo, you can mill the core by copying it exactly like doing an inlay/onlay. Its def more work in my opinion but can and has been done.
For anyone wishing to know how much radical decapitation of the tooth I performed, I submit the following images and radiographs.


During one of my weekls runs I thought about this tread.
It might be a different mentality that I sport but let me this:
For me these post are made for medical/scientific discussion. Sure the posts can be garnished with humorous remarks, and also also notes that do not fit to the case.
But for me I find it constructive if he says his open opinion about the matter as long as it is objective and constructive. This is valid also for counter-arguments.
Otherwise at least for me such a form looses some of it‘s value.
Why is that damn Kraut not posting his own cases so we can tear it apart as he does it with ours?