Why I Like Using the Articulator Function When Doing Implants

I just wanted to post some screen shots from a screw retained implant case that I just finished last week. I try not to have too much lateral function on implant restorations. I just always was taught that function down the long axis of the implant would be tolerated better long term and hopefully improve longevity. This case has 3 implant retained crowns. I did 13 and `14 a few years ago and 12 was a crown on a natural tooth. the tooth had very little support and I tried to convince her to get 3 implants or 2 and a bridge but she wanted to try and save it. 12 fractured to the gumline and she ended up getting that 3rd implant. When I image for implants I now image across to the contralateral canine because I have found using the articulator function has really helped to dial in my occlusion and eliminate these potential lateral interferences. Here is the scan and the intial proposal and some work I did on it from both straight on and from the occlusal shot.
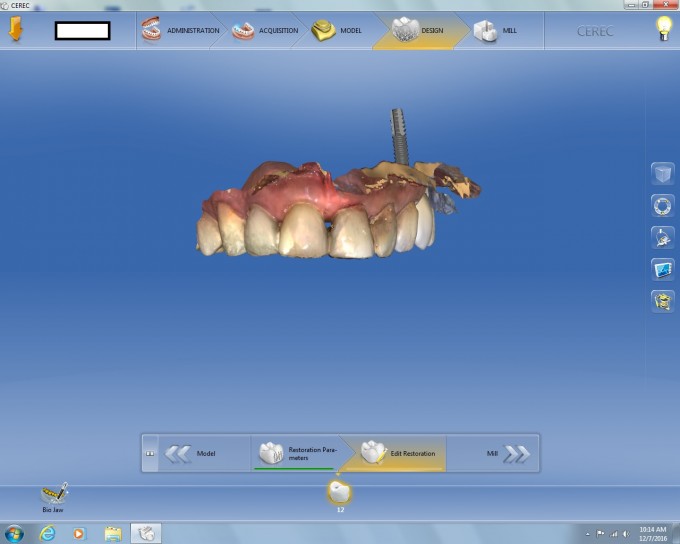
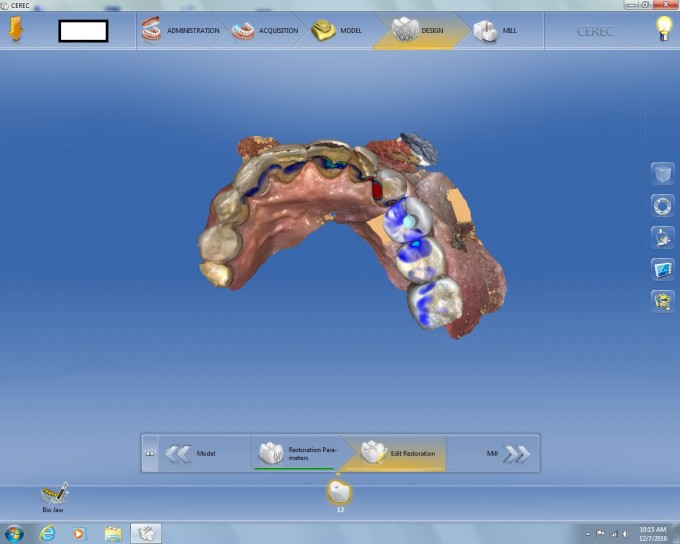
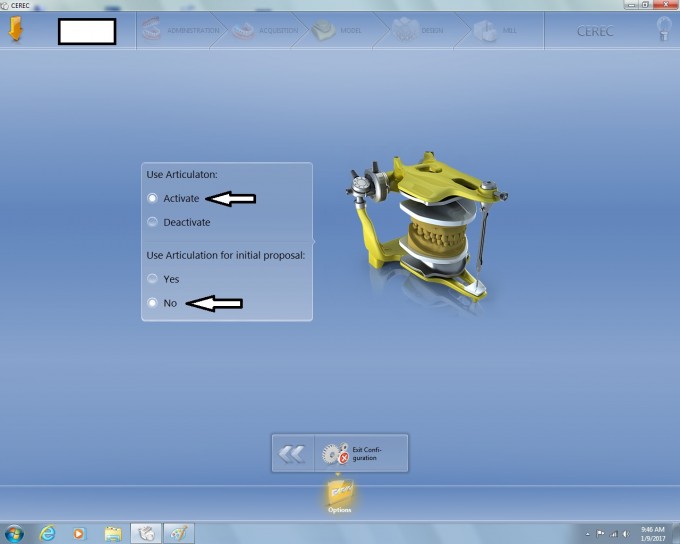
as you can see from the image from the occlusal view, I took the occlusion to a navy blue and removed all the maximum intercuspation interferences that I could see. Normally this would be pretty perfect, but sometimes I'd have to adjust some excursives. I decided to look and see if I had any excursive interferences. to activate the articulator, first you must activate it in the configurations. here are some screen shots of how to find it. Configurations-->options--->articulation once in there activate the options for the articulation but not to use it on the intial proposal. I found this really takes a long time to process and I don't need it for every case
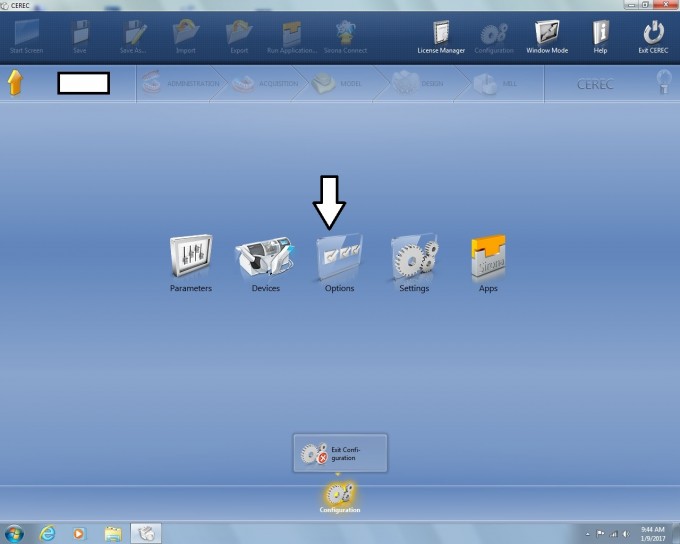
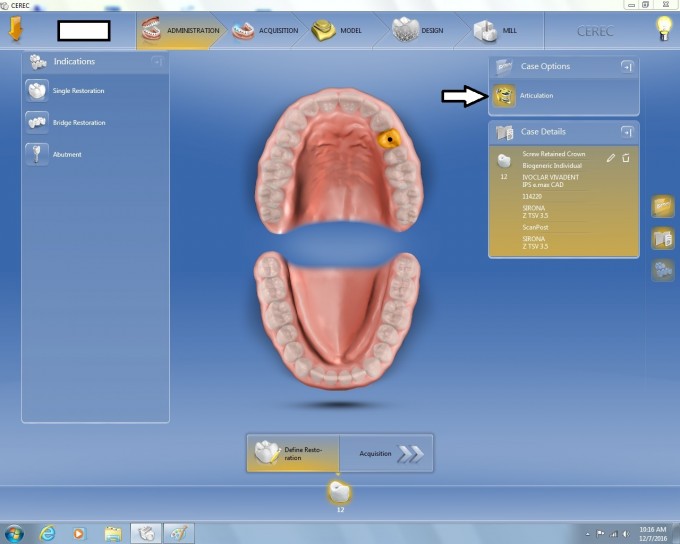
Once I you have activated the articulation in the configuration, you can select it for any case. In this case, after the proposal I went back to administrationan and clicked on the articulation icon and it then activates it
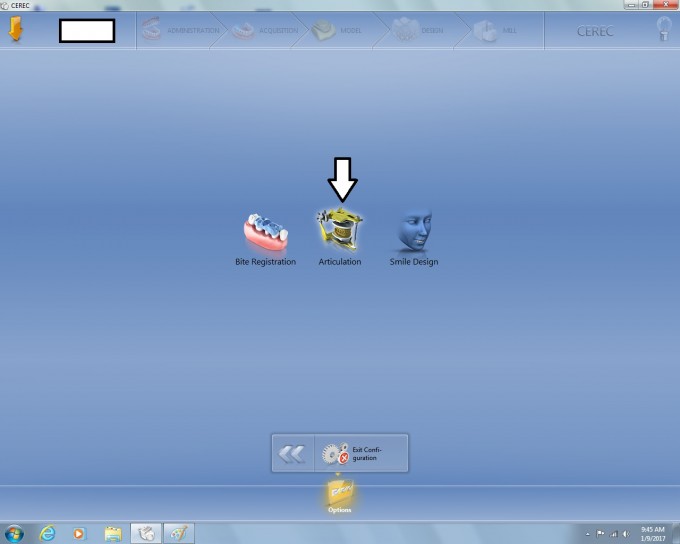
 Once I do that I click on the articulator icon in the design page and it will show my any excursive prematurity with the occlusal compass. In this case I was hitting near the cusp tip on the incline of the occlusal table above the screw hole.
Once I do that I click on the articulator icon in the design page and it will show my any excursive prematurity with the occlusal compass. In this case I was hitting near the cusp tip on the incline of the occlusal table above the screw hole.
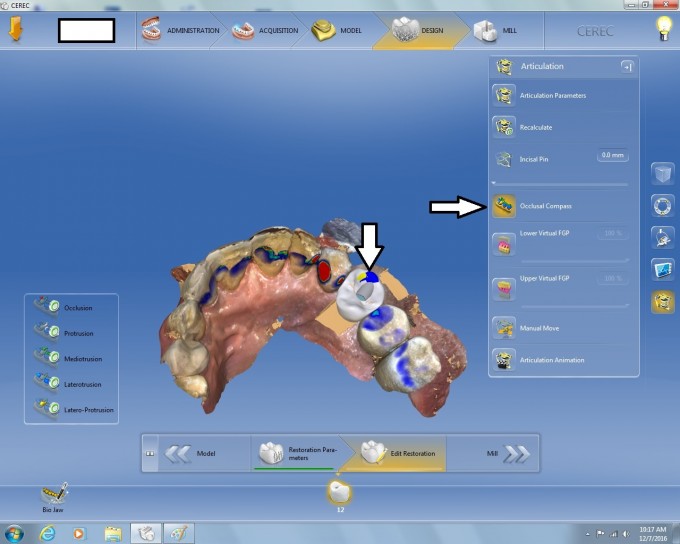
I can then just use my circular shape tool to remove this interference and have a restoration that I did not have to do any adjustment to other than polishing the composite over the access hole.

This does not have to be used only for implants but its when I tend to use it most. If you plan on using it, just make sure you image to at least the contralateral canine to give the software the necessary info to get us the most accurate results. Hope this will help you dial in your implants and bigger quad type cases.





Yep.... nice illustration Rich. @ Thad- need the contralateral canine as Rich noted. Primarily as this allows you to set the model axis correctly (which we are recommending anyways for all cases) -- I don't think it's a function of having the canine functional contact, but that the models are at the correct model axis, and the setting of your virtual articulator all set the models as a facebow will conventionally...
Mark
On 1/9/2017 at 12:03 pm, Thad Vincent said...Do you need to image more of the opposing arch?
image both arches to the contralateral canine. I'm not 100% sure on this, and maybe skram can chime in, but I believe the data points of the contralateral canine are used to help determine the excursives, just as in the mouth.

What Parameters are you using?
I think Mike said that the key to the movements was the midline point of the incisors for movement and setting the arch into the articulator.

Rich,
I have procrastinated using the Virtual Articulator because of simple lazy inertia. I am going to make a late New Year's Resolution to start doing this. Thanks for posting.



I read this right after seating a screw retained implant crown. Had to make some minor adj for excursions. I went back and checked articulator and the marks where pretty close, great tip. Thanks
Seriously, what parameters will work like an arbitrary semi adjustable such as a sam3 or other similiar? Any one have an idea?

Imaging to the contralateral
canine is best Rich, but per a conversation with Albert Mehl (inventor), he said it's close even if you don't and his contention is that you always should use it. Correct me if I'm wrong Sam

Imagine to the contralateral canine also makes it easier to set the curve of wilson for proposals.

Proposals have been so much better since I started imaging across the mid-line and setting model access properly.
Rich thanks for showing this case, really doesn't add any time or effort to an implant design to do this. Saves so much time adjusting the case in the mouth. Worse yet, imagine if the excursive contact didn't mark perfectly on the nice glazed e.max. You might have a terrible excursive contact putting too much force on the implant leading to screw loosening, breaking, bone loss, or implant failure. Great tip!

Rich this is great! Thanks for the step by step!!
It's a snow day here in the NW so it's a perfect opportunity to make a handout

I'm trying this out for my first time in 10 minutes. Restoring #30 screw retained. Activated and ready. Thanks for the post Rich and comments others


Rich, Quick question. I see that you do not have contacts on the contra-lateral premolar or canine. My biggest frustration, as with most cases that I scan over to the other side, is getting those contacts. I have used a couple of the techniques, such as taking anterior buccal bite at 90 degrees, with some success but never overly consistent. I am hoping that at some time they will give us the ability to get a bilateral buccal bite or allow us to toggle the initial model proposal so we can rotate the casts to get contacts on the opposing. I know we can scan in ortho and move over but the models come in as tan so on bridge cases the margination is more difficult. I have started to scan most of these cases with articulating paper marks on the contra lateral so I have some visualization. What technique has been most successful for you?

On 1/10/2017 at 6:15 pm, Michael Skramstad said... Imaging to the contralateral canine is best Rich, but per a conversation with Albert Mehl (inventor), he said it's close even if you don't and his contention is that you always should use it. Correct me if I'm wrong Sam
correct

On 1/11/2017 at 11:17 am, Michael Mingle said...Rich, Quick question. I see that you do not have contacts on the contra-lateral premolar or canine. My biggest frustration, as with most cases that I scan over to the other side, is getting those contacts. I have used a couple of the techniques, such as taking anterior buccal bite at 90 degrees, with some success but never overly consistent. I am hoping that at some time they will give us the ability to get a bilateral buccal bite or allow us to toggle the initial model proposal so we can rotate the casts to get contacts on the opposing. I know we can scan in ortho and move over but the models come in as tan so on bridge cases the margination is more difficult. I have started to scan most of these cases with articulating paper marks on the contra lateral so I have some visualization. What technique has been most successful for you?
Image like you do in Ortho. In that, do occlusal scan, lingual scan and buccal scan. Even do a couple of "transverse" rolls. Doesn't take that long and it seems to "construct" the models better where a buccal bite will stitch true. It apperas it's not the bite or the position of the bite but the construction of the models.