budget sensitive 91 Year old

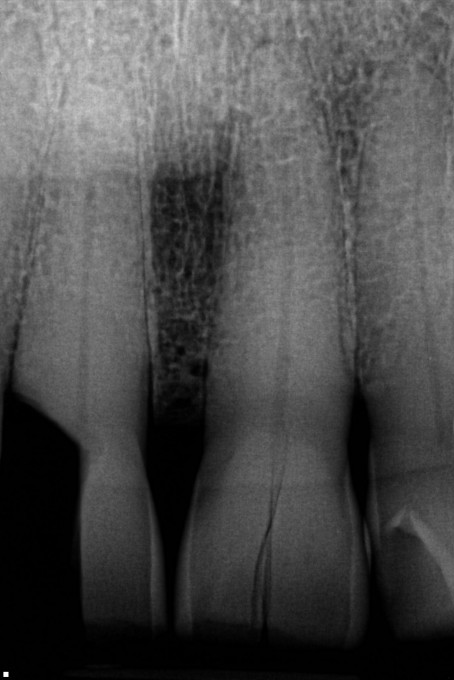
He broke the distal half of his central off into the attachment, crestal area. None of these teeth respond to cold, including the broken tooth. No teeth are tender to percussion.
He wants a simple solution and I'd like to provide him with one. I can do a composite restoration and hope for the best. I'm concerned though that I'm gonna cause gingival inflammation by violating the biologic width and/or a periapical abcess. What do you think is the right call here? I think I need to address the other central as well before the same thing happens.

You might try some of these cheaper but good blocks like GC America's CeraSmart. Just mill and polish.

These kind of cases have a habit of coming back and biting you in the butt if you compromise on what you know is best. I would say that if he wants the simplest solution, just pull the tooth, but I don’t think that’s what he means by a “simple” solution:) what happens if you make a beautiful Cerasmart crown, and the tooth develops an abscess or fracture off at the gum line? Do you refund the treatment that failed or do more treatment for free? I understand the desire from both the patient and the doctor to do “conservative “ treatment, but sometimes herodontics ends up costing more money and taking more time to get right. I don’t mean to preach, I’ve just been there so many times that I feel it’s not worth it taking shortcuts on these kind of cases.

Saw some Bioclear yesterday wich might help this case
Given his age if he's having no pain and no obvious pathology-"what would I do if this were my dad"........thinking.............I think I'd do a direct composite with some theracal/biodentine on pulp and wait and see.

Seems like as long as you inform the patient as to possible bad outcomes from doing minimal, conservative treatment--ie composite--then it's his decision to make and I wouldn't be too concerned. If it was my decision, as a 91 year old I would rather have a front tooth with gingival inflammation than no tooth. Do the treatment now and worse case you are having the conversation again in 6 months or a year when/if it begins to abcess.

If this situation walked into my office. I would offer him the same treatment options that I would a 30 year old. I would explain that his best treatment is extraction and replace with implant, bridge, partial, etc. If he wants to hold onto what is left and do it budget friendly, I would explain to him the guarded to poor prognosis due to the fracture extent and the proximity to the pulp and then I would go the composite route.
I had a similar situation, though not as severe a fracture, last year. I used a wide greater curve band to seal off below the fracture, bleach scrubbed and placed durelon over the pulpal area. Then restored using surpass and composite. Fingers crossed, but its still holding strong. Have a great day.
-Chad

I'm with Dan, prepare for it to last not to Maybe last. I'd look at RCT/Post & core/Crown. And yes, I'd try to get him to address #9 too. Of course an implant is an option as well as a flipper, but I'd be up for trying to save the tooth.
JJ

Why not extract 8 and do a 2 unit cantaliever off of 9. Solves both issues and is more predictable long term. What is he doing to fracture them in the first place?
I think were gonna do a traditional 3 unit bridge. After pondering overnight, Do it properly once prevails....

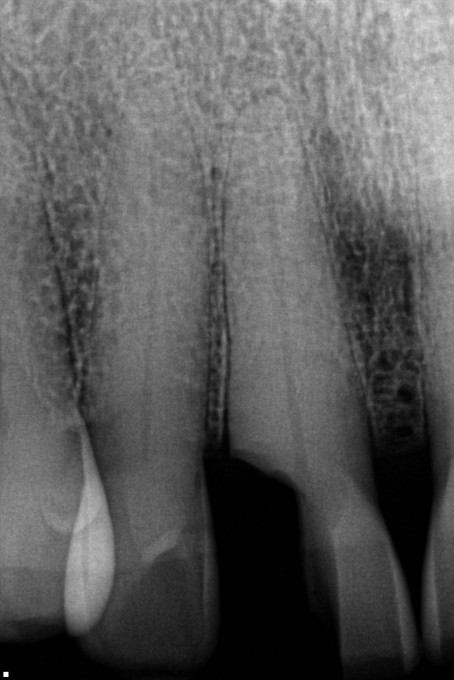
1-1 (#8) looks too far gone. I worry about the 2-1 (#9). That's a nasty looking vertical fracture. Given his advanced age, and the lack of any real dental care in a retirement home (should he be going to one in the conceivable future) I wonder if a flipper might be more prudent? Just a thought. I'd also have his name put into the flipper- those things go walking in the nursing homes!
TK, you're throwing a wrench in my plan! I like the idea. I started treatment this morning. He is remarkable for a 91 year old. He broke the tooth chewing on a hang nail. As it turns out, the nerve was open and necrotic. Once he was under anesthesia my explorer went into the canal without resistance. No bleeding. I Milled a cerasmart to rebuild the tooth and drew the distal margin on the gum. The actual fracture margin is deep and I want to make sure this part is as easy to recover from. I did a pulpectomy and put an intraoperative dressing. Now he's able to smile for a party he has this weekend and I have a a good mock up.
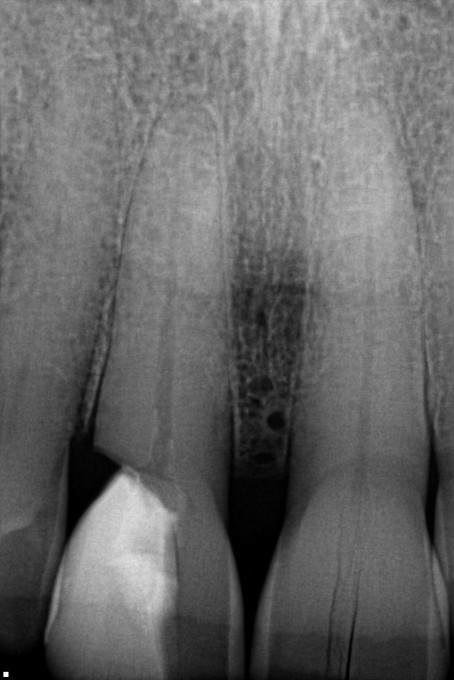
The plan is to prep for a FPD, send him to a surgeon for exo and then final impressions. Here's what the end of tx looked like today.


On 3/2/2018 at 8:49 am, Thomas Kauffman said...Crown lengthening is probably not a good idea due to the deficiency of bone between the central and lateral incisor. Just where would you stop you osteoectomy? Since the tooth is necrotic, I would consider perhaps doing the endo, fibre core post, and restoration. I think you have to consider the other central, and address both at the same time. If the other tooth had endo as well, I might consider 2 restorations splinted together. My thinking would be long term at 91, and he could well live another 10 years plus like my wife's aunt who passed at 104. Lots of options. please post the result as it is very interesting with options to consider.
This, and use either a strong fiber post or consider a metal one. After endo and a crown prep there will be very little remaining dentin to resist horizontal fracture of the remaining tooth so the post is necessary in this case. I would also consider margin elevation using something such as Geristore or Biodentine for compatibility with bone and connective tissue.


On 3/2/2018 at 12:10 pm, John Lee said... Ortho (Forced Eruption), RCT, P&C,CRN?
On a 91 year old who wants to fix it cheap? Really? zyou've got to be kidding. You need a dose of reality.

What is „budget sensitive“ in numbers? Did you ask him what he is ready to spend?
Maybe a revolutionary question: How much worn are his anteriors? Does he need this tooth for esthetics?
If yes, I would do the endo, then fiber post and the composite filling the best I could. I would consider the inflammation then the minor problem. And if it will create bigger problems on the long run he might be ready for better options.
I guess it‘s good to see it mainly from the patient‘s perspective in such a case. The patients at this age rather often do not care much about perfection in my experience, since they do not like the stress and the „unnecessary“ expense.
Charles. No. It is reality. I always present the options and choice to my patients regardless of age. I just referred an 82 year old lady for Ortho who wanted to straighten her teeth. She wanted to look good because she is now “single”. After many years of practicing dentistry, I realized everyone wants to hear all options. Second, forced eruption on anteriors are pretty predictable.
Well, Thomas, there was „budget sensitive“ explicitly written in the title line.
It was not repeated explicitly (and why should it if mentioned once?) in the text, but „simple solution“ will certainly imply it.
Sure you can present also an older patient the whole variety of modern dentistry.
Certainly not all older people are opposing it and some of them just need an awakening kiss.
Well, Thomas, this budget question was the one that I had mentioned ago.
So the game had changed. An anterior bridge is nothing that would deserve „budget sensitive“ in the headline. I did not know what the abbreviation „FPD“ means.
The ethical question was not touched at this point. The initial clear condition defined by Jason was low budget. This implied for me that he already had given all the information needed for this case and the patient had decided for low budget. And that was to respect.
Thomas,
I‘m not sure if you got my point: you are not treating a patient here but just answering Jason‘s question which premised that he had already taken care of all informative and other ethical obligations.
And it was not up to you to question that.
The initial only theoretical question was how to treat such a case on a low budget basis.
Will do. I was enjoying the Grand Tetons in Jackson Hole and was not following the evolution of this thread. I will keep you posted...back to work