Emax Custom Tissue Formers













Farhad, this may be a dumb question, but looking at the xrays it looks like implants were placed 1-2mm sub crestal in the initial xray. On the final xray implants looks like they are at bone level. Did you recontour the bone or is that bone remodeling by itself?
On 2/28/2017 at 3:55 pm, Mike Skramstad (Faculty) said...Just out of curiosity... why e.max? Price?
I still mostly use Enamic for these but I wanted to just point out another option in case someone does not have Enamic in stock. We can use Emax instead and not crystallize it to save that time. We still polish these slightly. Enamic mills faster but Emax is a little cheaper....Just another option.
Farhad
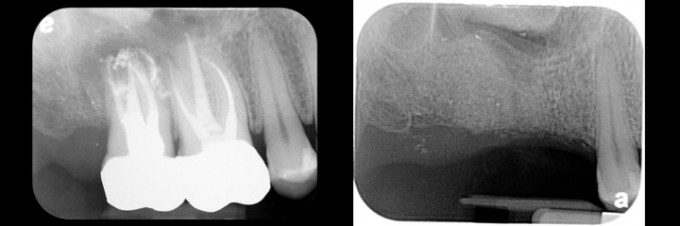
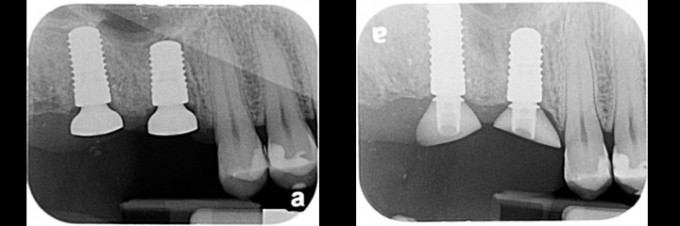
On 2/28/2017 at 4:04 pm, James Kim said...Farhad, this may be a dumb question, but looking at the xrays it looks like implants were placed 1-2mm sub crestal in the initial xray. On the final xray implants looks like they are at bone level. Did you recontour the bone or is that bone remodeling by itself?
Excellent question James and both you and Sam are correct:
If tissue formers placed at the time of surgery: Recontour the bone via profilers initially (enough to seat standard healing caps but usually not enough to seat customized tissue formers) and then contour bone additionally with diamond burs (to be able to seat customized tissue formers or even the standard Contour Healers).
If tissue formers placed after initial healing such as in this case: Recontour the bone via profilers only (to seat standard healing caps), bone will remodel on it's own during the healing time (~2months), and no further need for bone recontouring to seat customized tissue formers.
My current workflow in the majority of posterior cases:
1.) Place implant (s), use bone profilers to profile bone, place scanbodies and take CEREC scan, place standard healing caps and dismiss patient
2.) Fabricate customized tissue former (s) during the 6-8 weeks healing time
3.) At the 6-8 week post-op appointment remove standard healing caps, place compounded topical anesthetics, place customized tissue formers
4.) Start final restorative phase after 2-4 weeks (in our case refer patient back or in your case do it yourself)
Advantages: Save surgical appointment time, Easier tissue adaptation to standard healing caps during surgery, Time to work on fabricating customized tissue formers without stress, Bone will typically remodel and tissue can easily be displaced after 6-8 weeks as long as bone is initially profiled (unless bone is very very cortical).
Farhad
Farhad- IF (and its a big IF) there was a material that we could mill in 5 minutes and at minimal cost, you would make the custom formers at the time of surgery correct?

On 2/28/2017 at 4:35 pm, Farhad Boltchi (Faculty) said...On 2/28/2017 at 3:55 pm, Mike Skramstad (Faculty) said...Just out of curiosity... why e.max? Price?
I still mostly use Enamic for these but I wanted to just point out another option in case someone does not have Enamic in stock. We can use Emax instead and not crystallize it to save that time. We still polish these slightly. Enamic mills faster but Emax is a little cheaper....Just another option.
Farhad
Farhad, I would not use non crystallized e.max especially at surgery site, it is not strong enough and patient might easily break it and it will damage the site.
Sam, you can make a custom block from your favorite composite or acrylic and mill it.
The most cheap and fast way to accomplish this is to use flowable composite on a temporary abutment. Gregory

Gregory
Can you site even one clinical example in which that has happened? I would be shocked
Making a custom clock out of acrylic = waste of time and not much savings. I did this like 10 years ago.
Plus no custom fit to tibase. It's a total waste of time IMO
There will be a better solution in future I'm sure if it
On 2/28/2017 at 7:17 pm, Michael Skramstad said... Gregory Can you site even one clinical example in which that has happened? I would be shocked Making a custom clock out of acrylic = waste of time and not much savings. I did this like 10 years ago.
Mike, Sam was asking about cheapest block to mill for 5 min. I just gave an example. I do not do that but have seen the cases
The cases I refer Mike when you do immediate implant placement and socket shape is used as shape of abutment. Gregory
On 2/28/2017 at 5:35 pm, Gregory Mark said..The most cheap and fast way to accomplish this is to use flowable composite on a temporary abutment. Gregory
You are missing out on the biggest benefit of a custom healer made by cerec. On the second visit your final restoration is already done because you made your healer from your full contour restoration.
On 2/28/2017 at 8:24 pm, Sameer Puri said...On 2/28/2017 at 5:35 pm, Gregory Mark said..The most cheap and fast way to accomplish this is to use flowable composite on a temporary abutment. Gregory
You are missing out on the biggest benefit of a custom healer made by cerec. On the second visit your final restoration is already done because you made your healer from your full contour restoration.
Agree! Gregory
On 2/28/2017 at 5:35 pm, Gregory Mark said...Farhad, I would not use non crystallized e.max especially at surgery site, it is not strong enough and patient might easily break it and it will damage the site.
Sam, you can make a custom block from your favorite composite or acrylic and mill it.
The most cheap and fast way to accomplish this is to use flowable composite on a temporary abutment. Gregory
Gregory,
I have not seen this in any of the cases we have done over the past 2 years. Remember these tissue formers are at tissue level so unless the patient places a jolly rancher vertically in there and bites down I doubt these would ever fracture.
Farhad
On 2/28/2017 at 5:23 pm, Sameer Puri said...Farhad- IF (and its a big IF) there was a material that we could mill in 5 minutes and at minimal cost, you would make the custom formers at the time of surgery correct?
Enamic mills pretty fast but it still takes time to design, mill, bond to tibase, polish. Our fastest time has been 35-40 minutes.
My ideal option would be: Scan at the time of surgery, design and mill a one-piece tissue former out of a material such as peek, polish....with a total time at 15 minutes.
Second best ideal option: Being able to design and mill the tissue former prior to surgery.
Farhad

Can place a contour healer and shape it to ideal and place a week 6-8. If this is in the posterior your final restoration will be close enough to deliver final restoration (assuming took cerec scan at placement). Cost $40 and you haven't burned a tibase and emax abutment block ($140).
I agree though - I wanna mill peek in office

If we're talking cheap and time efficient, make them prior to surgery with the cheapest block you can (this might be a left over section of block from milling a regular Cerec restoration -effectively costs you nothing!) The tiBase can be reused for the next healing cap you make, so again cost neutral.
I've been milling individual custom abutments for healing caps for a few years now and honestly, I'd say they all fall into maybe a dozen different shape/forms. Plus they cost about 5-10 dollars each. Which is why Trey's contour healers work - because the average implant crown can be made from the the average contour healer if the implant is placed in the average location (ie : centred in the edentulous space).
So, a couple of ideas...keep a watch on your custom healing cap shapes. You might be surprised to find they all end up pretty similarly shaped over time when you compare all you molars, all your premolars, all your incisors, etc to each other. Of course there will always be subtle differences.
To save surgery appointment time, if you want to have something ready pre-implant placement, make up a dozen or so doughnuts of ceramic from any old block piece or type to fit a tibase. (Scan the tibase on your desk/lab model and design your average molar healing cap profile on it , calling it a canine crown for the sake of the software).
Once you have placed the implant add a tibase, then try on the doughnuts until you find one that gives you your ideal(or close to) form, take the tibase off and glue the ceramic on and you're done. 5 mins tops at time of surgery. Ok, if you don't have a shape quite right, either cut it back with a highspeed or go plan B and mill up an Enamic on the spot - 30 mins as per Farhad. ...so now you have your "off the shelf" custom healer ready, take a scanpost of the implant, put the healer in and take a gingival mask and you have all you to make your final crown in a few months by simply copying the gingival contour of the healer.
There's no need to waste a meso block ($$) of any type by doing it this way as doughnuts of ceramic are under no load and do not dislodge - it's only anti-rotational. I'd agree too that uncrystalised Emax with a strength equal to Vita mark II should not be able to be fractured.

Farhad very cool stuff! Just out of curiosity what was wrong with those teeth? The RCT's look pretty good? Cracked roots? Anyway very nice stuff. I do however think there is some pre-IDS Meeting subliminal messaging going on here just like in the Midwinter scanner evaluation thread ;-) From Sam and Mike respectively. Looks like some interesting times ahead!
"Farhad- IF (and its a big IF) there was a material that we could mill in 5 minutes and at minimal cost, you would make the custom formers at the time of surgery correct?"
"Plus no custom fit to tibase. It's a total waste of time IMO
There will be a better solution in future I'm sure if it"

Farhad, please elaborate on this. 3.) At the 6-8 week post-op appointment remove standard healing caps, place compounded topical anesthetics, place customized tissue formers
I find even under local anesthetic the patient is still quite uncomfortable when trying to switch to a larger healing cap. I used to do it in slow increments with pauses in between but it's stressful on the patient and myself. I pretty much abandoned that and use a laser to widen the space for better emergence. However, if there is limited A.G. it's a problem.
On 2/28/2017 at 11:04 pm, John Daw said... Can place a contour healer and shape it to ideal and place a week 6-8. If this is in the posterior your final restoration will be close enough to deliver final restoration (assuming took cerec scan at placement). Cost $40 and you haven't burned a tibase and emax abutment block ($140). I agree though - I wanna mill peek in office
Contour healers are awesome and superior to the stock abutments. However, you dont get the advantage of being able to fabricate your definitive restoration prior to your second appointment. Your tissue will be close, but not exact. Maybe that matters, but its doubtful. The most important part is the time savings.
You will reuse the tibase from these so you only have the cost of the block but the bigger issue is the time it takes to make them at the first visit.
I completely agree with Sam. I always keep some contour healers in stock and use them when possible. Not a cost advantage to customized Cerec tissue formers except time. The 2 issues that prohibit me from using the contour healers more than I do are that they come only in one size, flare out laterally too quickly, and that they are indexed. They typically require more manual adjustment than I am willing to do.
Farhad
@Jason:
Make sure the bone has been profiled/adjusted adequately, take healing cap off, fill out the implant sulcus with TAC 20 or BestTopicalEver and then place some additional amount on the buccal and lingual peri-implant gingiva (no need to place any in the vestibule but just a good amount around the implant itself filling the area up), place a gauze on the site and have the patient bite down (to make sure they don't swallow any), leave the topical on for at least 5 minutes (average 5-7 minutes), place tissue former...they will not feel a thing.
Farhad
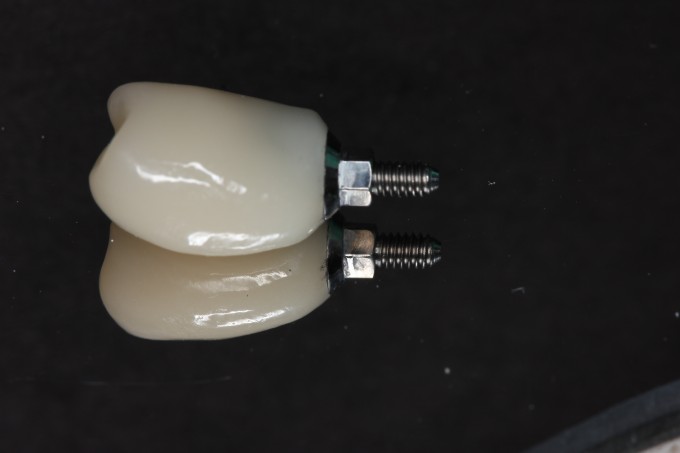
Here is the huge advantage of the custom tissue formers. This custom former is based on the contours of the screw retained temp. When this implant heals and the patient comes back for the second appointment, we can already have the screw retained temp made ahead of time because its made from the full contour restoration. It pops right in with no issue with the tissue:

This lab work can be done before the patient arrives:


On 2/28/2017 at 4:56 pm, Farhad Boltchi (Faculty) said...On 2/28/2017 at 4:04 pm, James Kim said...Farhad, this may be a dumb question, but looking at the xrays it looks like implants were placed 1-2mm sub crestal in the initial xray. On the final xray implants looks like they are at bone level. Did you recontour the bone or is that bone remodeling by itself?
Excellent question James and both you and Sam are correct:
If tissue formers placed at the time of surgery: Recontour the bone via profilers initially (enough to seat standard healing caps but usually not enough to seat customized tissue formers) and then contour bone additionally with diamond burs (to be able to seat customized tissue formers or even the standard Contour Healers).
If tissue formers placed after initial healing such as in this case: Recontour the bone via profilers only (to seat standard healing caps), bone will remodel on it's own during the healing time (~2months), and no further need for bone recontouring to seat customized tissue formers.
My current workflow in the majority of posterior cases:
1.) Place implant (s), use bone profilers to profile bone, place scanbodies and take CEREC scan, place standard healing caps and dismiss patient
2.) Fabricate customized tissue former (s) during the 6-8 weeks healing time
3.) At the 6-8 week post-op appointment remove standard healing caps, place compounded topical anesthetics, place customized tissue formers
4.) Start final restorative phase after 2-4 weeks (in our case refer patient back or in your case do it yourself)
Advantages: Save surgical appointment time, Easier tissue adaptation to standard healing caps during surgery, Time to work on fabricating customized tissue formers without stress, Bone will typically remodel and tissue can easily be displaced after 6-8 weeks as long as bone is initially profiled (unless bone is very very cortical).
Farhad
I had always understood that around 8 weeks the bone is undergoing some remodeling that is at its peak and that is not typically a time you would want to unscrew/screw things into the fixture. Is that not so?

I like tissue formers, but I have found the best way to get perfect fitting gingiva (posterior teeth) is to create an ideally shaped tibase/crown and at the time of delivery just make a small incision (mesial-distal) over the cover screw and then "tuck" the crown into the site and tighten it down. The gingiva will grow perfectly to the crown instead of trying to make the perfect crown that contours to the gingiva. Two appointments,1) place implant and take impression, 2) deliver premade crown. Works perfect everytime. Just a thought if you don't want to mess with the tissue healers.
On 3/1/2017 at 1:41 pm, Scott Donner said...I like tissue formers, but I have found the best way to get perfect fitting gingiva (posterior teeth) is to create an ideally shaped tibase/crown and at the time of delivery just make a small incision (mesial-distal) over the cover screw and then "tuck" the crown into the site and tighten it down. The gingiva will grow perfectly to the crown instead of trying to make the perfect crown that contours to the gingiva. Two appointments,1) place implant and take impression, 2) deliver premade crown. Works perfect everytime. Just a thought if you don't want to mess with the tissue healers.
Scott,
this is certainly one option and I like the fact that you are taking the scan at the time of surgery. My only concern would be that the final tissue level is not as predictable with this technique. I highly doubt that esthetically this is an issue in the back of the mouth but in the premolar area, and obviously the anterior area, this may lead to problems.
But again- I love the idea of taking the scan at the time of surgery.

Actually, some literature I've seen shows that the best tissue adhesion is to emax unfired, just polished.
On 3/1/2017 at 2:12 pm, Sameer Puri said...Actually, some literature I've seen shows that the best tissue adhesion is to emax unfired, just polished.
+1

On 2/28/2017 at 4:35 pm, Farhad Boltchi (Faculty) said...On 2/28/2017 at 3:55 pm, Mike Skramstad (Faculty) said...Just out of curiosity... why e.max? Price?
I still mostly use Enamic for these but I wanted to just point out another option in case someone does not have Enamic in stock. We can use Emax instead and not crystallize it to save that time. We still polish these slightly. Enamic mills faster but Emax is a little cheaper....Just another option.
Farhad
Brilliant Option! I agree that e.max is less inexpensive and for that purpose, I agree 100%.

Farhad,
At what time do you replace healing cap with contoured healer and how long do you keep in place before final restoration? Also what do you charge patient and do you code as temp abutment and temp crown?
Thank You
On 5/16/2017 at 2:14 pm, Jeffrey Clark said...Is there anyway you could post rst file for that case.
Here you go.
Farhad

Since the TiBases are modified in this technique, they may not always be re-usable from case to case. I think we just need an inexpensive plastic TiBase ?

On 11/14/2017 at 2:59 pm, Gary Walker said...Since the TiBases are modified in this technique, they may not always be re-usable from case to case. I think we just need an inexpensive plastic TiBase ?
We have been asking for that for eons!!!! Hopefully someday!!

On 11/14/2017 at 3:05 pm, Mark Fleming said...On 11/14/2017 at 2:59 pm, Gary Walker said...Since the TiBases are modified in this technique, they may not always be re-usable from case to case. I think we just need an inexpensive plastic TiBase ?
We have been asking for that for eons!!!! Hopefully someday!!
Yep... seeing the wish list in Sam's new White Paper too... a non-indexed less expensive tibase is also on that list
Mark

On 11/14/2017 at 3:05 pm, Mark Fleming said...On 11/14/2017 at 2:59 pm, Gary Walker said...Since the TiBases are modified in this technique, they may not always be re-usable from case to case. I think we just need an inexpensive plastic TiBase ?
We have been asking for that for eons!!!! Hopefully someday!!
1 M Flem...maybe print some...Id bet you and Pete could come up with that!