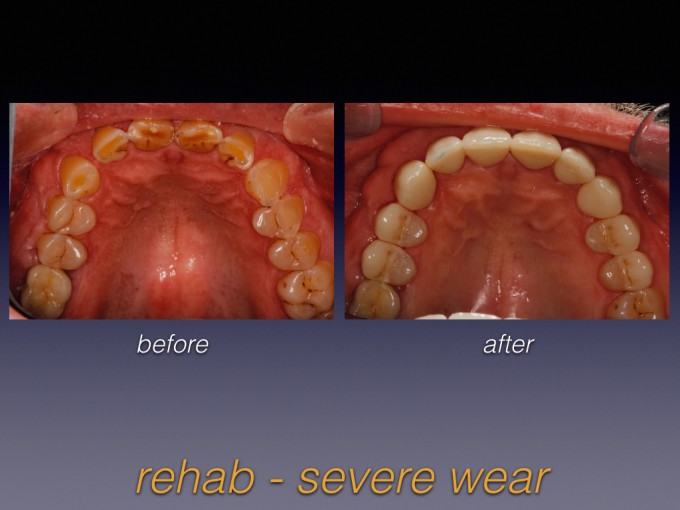
wear case

How do you go about determining which wear cases you can treat predictably? Is all tooth wear the same? If not, how do you decide how to treat? Here's a case to kickstart the discussion:



I love cases like this one and find them extremely rewarding. I also use Cerec as another way to increase predictablility in these cases...namely using strict Biocopy.


Ross,
Great case and outcome.
Very nice shape and characterization.
Making sure to recognize the etiology of the wear, and treat to avoid ANY interferences in motion is the main goal to longevity of these rehabilitations!!!
Great job.
It looks like you even added on to his beard. ![]()

Great outcome Ross! I'm looking at your post on my phone so tough to see. Looks like end-to-end wear and a lot of acid erosion. Generally a pretty safe and predictable restorative case.
Did you use a custom incisal table? Even though this doesn't look like pathway wear to me, it never hurts to maintain or open the existing envelope a bit.
Looking forward to learning more about this case. Especially what you mean by "strict biocopy". Do you change anterior occl offset parameters and leave occl offset in the posterior, etc?
Again, awesome job!


Just a beautiful result! It looks like you didn't change the verticle at all? What made you decide not to open the bite?

Beautiful result, and a GREAT service for the patient. Wear cases can be complicated if you don't know what is happening. Taking Spear courses makes it relatively much easier. I would definitely recommend that anyone interested in treating cases such as this take Spear. Ross is an excellent example of the synergy possible having taken both Cerecdoctors.com and Spear courses.
Winnie

Great case Ross. Have you used Telio CAD bridge blocks as an interim solution (test-driving the occlusion, phasing the treatment over time, etc.) to treat severe wear cases that require opening the vertical dimension?
The responses have been spot-on so far. You guys definitely had your coffee today! Here goes....
@Karen - Great question. I biocopied the provisionals that were derived from the diagnostic wax-up, adjusted intraorally, and esthetically approved. This is the key to predictability with Cerec in these larger cases. Test drive in plastic, then duplicate in ceramic.
@James - If I could grow hair, my friend, it'd be on my own head and not on this guy's face. Sadly, those powers evade me.
@John - a.) You are absolutely correct regarding the type and location of wear. It was erosive and end-to-end just as you suspected. b.) I also agree that, despite it looking scary, it's generally predictable to treat...although you can tell by the massive exostoses and his hypertrophic masseters that he is or was a bruxer. That's actually an entirely separate conversation and we could do an entire thread talking about bruxism vs. parafunction. c.) You also scored another hit with the custom incisal guidance table. Yes, I made one for the wax-up and the contours of the provisionals were shaped to be beyond his envelope of function. d.) Strict Biocopy just means that I did not allow the software to propose any of the functional surfaces and I controlled the entirety of the final occlusion via Biocopy of the provisionals. Anterior offset was 0 and posterior offset was my usual -175.
@Daniel - Once again, you guys are very sharp and you are correct that I did not change the vertical. Why not? I didn't need to because his VDO hadn't changed (there was no molar occlusal wear so there could have been no loss of vertical) and it wouldn't have helped the function or esthetics of the case either. I didn't change VDO and, as John astutely pointed out, I didn't deepen the bite...so how did I gain restorative room to make the teeth longer? I'm sure you guys can figure out what I did! Just think about the case goals, the location of the wear, and how that wear affected his dentition. Those are the clues to best figure out how to put back what he lost (hint, hint...and it's not VDO).
@Askold - I totally agree with the Spear comment. The Worn Dentition workshop and seminar was one of the most interesting and applicable courses I've ever taken. I practice in Florida, so I see a lot of old, failing occlusions and a lot of tooth wear. Spear has given me the foundation to understand, diagnose, and predictably treat tooth wear. (http://www.speareducation.com) And even with all that, it's still hard to do!
@John - Actually, I have not done that but I'd like to try. There's one major drawback that I can think of, though. It doesn't apply to this specific case, but follow me for a second here. One trick I've learned to increase the accuracy of articulator-mounted cases for your diagnostic wax-up is to take the CR record (Leaf guage is my preference) at the VDO that you expect to build the case, NOT the patient's existing worn VDO. Essentially, you want to record the distance you intend to open the patient as part of your initial mounting. On the other hand, if you take "the bite" at the existing/reduced VDO, you then have to open the pin on the articulator to accomplish your wax-up and, depending on things like the accuracy of the facebow mount relative to joint position/rotation and how "average" your patient is, you have now just introduced an unknown degree of error. I hope that makes sense so far. Point is, I'm not sure what influence all these things will have on a virtual articulator and whether or not the software could even record a leaf-guage/CR/seated condyle bite that has no tooth-to-tooth interarch contact. On the majority of cases, it wouldn't matter, but if you wanted to change the VDO (aka "open the bite") it could have a major effect and seriously reduce your virtual accuracy of the real occlusion. And if you're going to all the trouble to mill overlay provisionals, the last thing you want to do is to have parts of it out of occlusion and other areas in hyperocclusion. I'd much rather grind or add to Bisacryl for the time being.

Ross,
Great case. You nailed this. I am thinking this is what you saw. Let me know if I am on course. Little posterior wear/signifcant buccal erosion. So I am assuming you got him into CR. Found that you had more space then you would think. Eliminated the any interferences that may have postured him forward and restored from there. Looks like you only added to the upper premolars to take care of the deficient buccal corridor. Corrected guidance. I love these cases because the intial impression before model is that this is a full mouth case. Once you start putting together some of Spear ideas you find that you were able to be much more conservative on your approach. Great case to share and discuss.

On 8/10/2015 at 3:15 pm, Michael Mingle said...Ross,
Great case. You nailed this. I am thinking this is what you saw. Let me know if I am on course. Little posterior wear/signifcant buccal erosion. So I am assuming you got him into CR. Found that you had more space then you would think. Eliminated the any interferences that may have postured him forward and restored from there. Looks like you only added to the upper premolars to take care of the deficient buccal corridor. Corrected guidance. I love these cases because the intial impression before model is that this is a full mouth case. Once you start putting together some of Spear ideas you find that you were able to be much more conservative on your approach. Great case to share and discuss.
Michael, you got part of it right. There was a CR to CO adapted shift that gained me some anterior-posterior room, but I still needed to find vertical room. A close look at the lower anteriors should give you the answer.

On 8/11/2015 at 9:10 am, Anthony Ponzio said...Did you retrocline them in the final restorations?
Slightly, but that wasn't the important part. Does this photo help?...

On 8/11/2015 at 9:18 am, Ross Enfinger said...On 8/11/2015 at 9:10 am, Anthony Ponzio said...Did you retrocline them in the final restorations?
Slightly, but that wasn't the important part. Does this photo help?...
Looks like you orthodontically intruded the lower anteriors from what I am seeing from the intial photos.
Exactly, Michael. I actually kept the same lower incisal plane on the restorations as he had on his worn teeth. Since they had supraerupted so much, we intruded them 3-4mm to gain the room I needed to restore them back to their correct heights. As you can see in the last photo I posted, it's very difficult to get pure intrusion...so you will note that the cuspids extruded a little during the orthodontic process. But I have to say that my orthodontist did a phenomenal job of preventing them from flaring as he intruded them.
On 8/11/2015 at 11:53 am, Daniel Butterman said...I thought this case was cool before, but ortho intrusion as well..... Amazing job!
Thanks, Daniel. The ortho was integral to the success of this case. Our tendency is to see a lack of restorative room and assume that we need to open the bite to gain it back. Sometimes that's the case, of course, but not always. It really depends on the esthetics of the incisal edges of the upper and lower anteriors and whether the wear occured on all the teeth or just some of them. In this case, he had been told repeatedly that he needed full mouth rehab to open the bite. But his tooth wear was segmental only, with no molar wear and heavy anterior wear with supraeruption of the lower anteriors. I explained that FMR was an option, but he could easily treat fewer teeth and get a better esthetic result if he were willing to have ortho to intrude the lower incisors. Amazingly, his wife is a former ortho assistant, yet this had never been offered as a possible plan! Needless to say, they jumped on that option and he was able to spend half the cost in my office than they had planned. Maybe not the brightest business decision on my part, but it's more important to do the right thing for the patient...plus it's a great practice-builder with patients and reputation-builder with your specialists.

On 8/11/2015 at 9:18 am, Ross Enfinger said...On 8/11/2015 at 9:10 am, Anthony Ponzio said...Did you retrocline them in the final restorations?
Slightly, but that wasn't the important part. Does this photo help?...
Those tori are impressive. Does he have any anterior guidance now? What happened to the UL premolar?
On 8/12/2015 at 8:20 am, Adam Langan said...Those tori are impressive. Does he have any anterior guidance now? What happened to the UL premolar?
So this is a good case to discuss guidance schemes. After taking a thorough medical and dental history, I think he had gastric reflux at some time in the past and that reflux triggered nocturnal bruxism. The acid erosion destroyed the teeth (with more damage happening on the right side) and the bruxism accelerated the erosive wear. However, the reflux and bruxism eventually resolved. Why do I think this? Look at his upper incisors...there are jagged edges of enamel that would never survive if he were still bruxing on them. Also, he had shoulder surgery several years ago and can't sleep on his right side (where there is more GERD damage), so I inferred that the acid damage is old. I also had him in temps for several weeks and we had zero issues.
That being said, I still hedged my bet by setting up an occlusal scheme that minimizes his chances of breaking things. For example, this is not a patient that I'd put in steep cuspid guidance. I designed the excursive movements with shallow guidance, group function on the cuspids and first bicuspids, and smooth crossover to the incisors. This scheme intentionally increases the contact areas on ceramic to spread out the occlusal load.
As for #13, he had endo/perio issues from the moment I saw him. We treated the endo but the J-lesion never resolved. My periodontist just extracted it and placed an implant which we will restore in a few months.