U/L overdentures using CEREC-GALILEOS

There is so much that we can offer and do for our patients utilizing the CEREC & Galileos. The greatest advantage is the ease, planning, and predictability the integration offers for implant placement. These procedures (whether single or multiple units) are now a stress-free appointment, and something that we, as general practicitioners, can perform. I'm no Farhad Boltchi by any means, so I only tackle the cases that I am confident and comfortable with. The following case is probably the most challenging case I've treated so far and was completed last month. The surgical and restorative phases were all completely in my office.
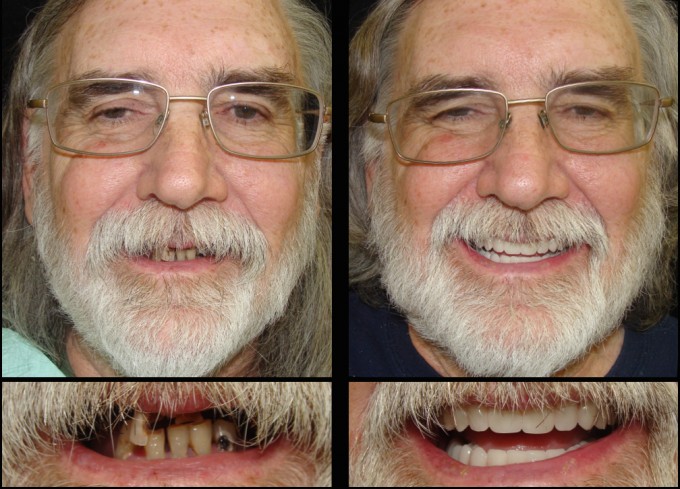
The patient is 63 years old, and he presented with rampant decay and periodontal issues in the few remaining teeth that he had. His primary goal was to be able to eat a steak again. Because of the hopeless condition of his teeth and in order to achieve optimal esthetics and function, we decided on extracting all of his teeth, and based upon his finances, he elected to proceed with implant-supported overdentures. We started the planning in October 2014, performed the surgery in November 2014, and restored the case in July 2015.
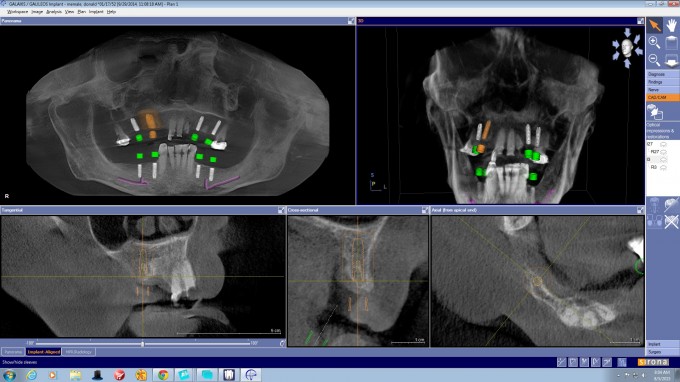
The planning involved comprehensive oral examination, radiographs/3D-scan, study models, facebow transfer/Sam3 articulator and digital photographs of the patient (intraoral/extraoral). All these were used to aid in a FGTP (Spear) approach.
The surgery was performed in 2 separate visits (upper arch versus lower arch and 3 weeks apart from one another). Because the patient's remaining teeth were stable, I was able to use a tooth-supported optiguide. So, we actually placed the implants first, then removed the teeth, performed about 2-4mm of bone reduction and grafted (in that order). Immediate dentures were delivered to the patient.
The restorative phase involved remounting the case using a new facebow transfer. From there, we fabricated new U/L overdentures using locators and improved/corrected any esthetic/functional concerns that were present in the immediate dentures.
The patient was very happy with his new teeth and could not believe he could smile without inhibition, talk with confidence and eat without pain. This case has probably been one of the most rewarding cases I have done so far. If it were not for the CEREC-Galileos integration, I definitely would not have been able to.






Thanks guys! Still learning and can't wait to tackle more difficult cases after I take Garg's advanced course.




Great presentation and explantion . I wish I could do that like you !
You made this comprehensive case look easy.

Really a fantastic result! Did you place any sort of framework into the dentures? I find sometimes the locator attachments can be a point of denture fracture over time without some denture reinforcement.

On 8/6/2015 at 12:03 pm, Daniel Butterman said...Really a fantastic result! Did you place any sort of framework into the dentures? I find sometimes the locator attachments can be a point of denture fracture over time without some denture reinforcement.
Daniel brings a good point here, the upper overdenture with locators on the upper arch seems to bring a lot more maintenance and complications; I don't know if this is the answer but splinting the implants on the upper arch has worked better for me;
Nevertheless, nice case from start to finish! great planning and execution!


Very nicely executed and documented case John.
I have mentioned this previously but the dentists that combine SPEAR and CEREC just take their dentistry to whole different level.
Farhad

On 8/6/2015 at 1:02 pm, Rodrigo De Marco said...On 8/6/2015 at 12:03 pm, Daniel Butterman said...Really a fantastic result! Did you place any sort of framework into the dentures? I find sometimes the locator attachments can be a point of denture fracture over time without some denture reinforcement.
Daniel brings a good point here, the upper overdenture with locators on the upper arch seems to bring a lot more maintenance and complications; I don't know if this is the answer but splinting the implants on the upper arch has worked better for me;
Nevertheless, nice case from start to finish! great planning and execution!
That's de idea I got, but never really saw any evidence or literature. The guy that does the surgeries for me always ran away from it. He does fixed or nothing at all. The cost of a bar with locators is the same of a hibrid, so he goes for the latter.
What is your long term feedback on free standing locators vs bar with locator? I'd like to propose more treatments like this (since they are cheaper to the patient) if I knew it works in the long term.
love the outcome of your work!!

On 8/6/2015 at 10:07 pm, Farhad Boltchi (Faculty) said...Very nicely executed and documented case John.
I have mentioned this previously but the dentists that combine SPEAR and CEREC just take their dentistry to whole different level.
Farhad
Graet work John,
Between seeing Ross's and your presentations I'm thinking SPEAR must have a lot going for it. Can't say I have a clue what SPEAR is, but I'll have to look into it.
Damian,
SPEAR is the other half of the Scottsdale Center educational facility. Their curriculum is based on the teachings of Frank Spear, a Prosthodontist, who is hands-down the best educator in dentistry worldwide. Their curriculum is heavy on treatmemt planning and actually understanding why instead of just the how.
Combining that knowlredge with the CEREC digital technology is a "deadly" combination as Ross put it.
Farhad

John,
Very nice end result and nice documentation. Thanks for sharing.
I'm interested in:
1/ how you decided what sites to place the implants
2/ how you feel about maxillary overdentures and long term implant success.
On 8/6/2015 at 1:02 pm, Rodrigo De Marco said...On 8/6/2015 at 12:03 pm, Daniel Butterman said...Really a fantastic result! Did you place any sort of framework into the dentures? I find sometimes the locator attachments can be a point of denture fracture over time without some denture reinforcement.
Daniel brings a good point here, the upper overdenture with locators on the upper arch seems to bring a lot more maintenance and complications; I don't know if this is the answer but splinting the implants on the upper arch has worked better for me;
Nevertheless, nice case from start to finish! great planning and execution!
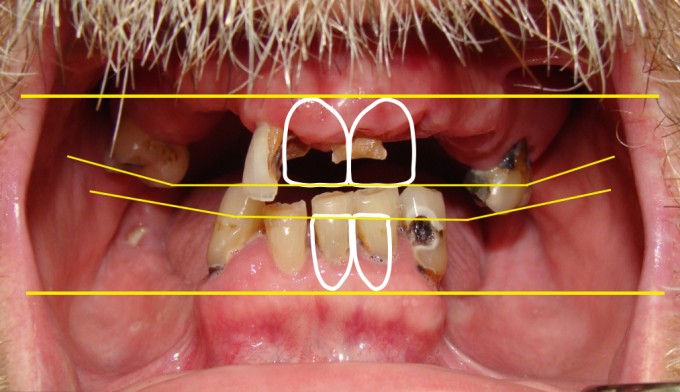
@Daniel & @Rodrigo. Thanks guys for the comments! So far, I haven't witnessed any issues or seen any research against using locators for maxillary palateless overdentures for long-term success. The key point that I've read in the research is having an adequate amount of restorative space from the platform of the locators to the incisal edge of the prosthesis. Obviously, this is crucial not just for the success of locator-supported overdentures, but also for Hader-bar overdentures and also for fixed implant-supported hybrids. I think this is why we see so many failures (whether it be functional, esthetic or hygienic) with any one of these three solutions. For this case, I did have to perform some bone reduction to meet the requirements for restorative space, but not nearly as much as what would have been needed for an "All-on-4" fixed hybrid. Those types of cases go to my periodontist. Also, other important factors that would influence long-term success are occlusal schemes/design, implant spread and cleansability.
I have to agree with John here.
I have been doing this solution (Maxillary overdentures on free-standing locators) for 15 years now, typically on 4 implants with a couple on 6 implants and a couple on 3 implants.
The only failure I have had was one case where I knowingly pushed the limits and placed 2 X 6mm implants for a locator-supported overdenture....Both implants failed after 2 years.
I know the issue with the concern for this type of treatment comes up again and again...I just have not experienced any problems with this solution.
Farhad
On 8/7/2015 at 10:33 am, Farhad Boltchi (Faculty) said...I have to agree with John here.
I have been doing this solution (Maxillary overdentures on free-standing locators) for 15 years now, typically on 4 implants with a couple on 6 implants and a couple on 3 implants.
The only failure I have had was one case where I knowingly pushed the limits and placed 2 X 6mm implants for a locator-supported overdenture....Both implants failed after 2 years.
I know the issue with the concern for this type of treatment comes up again and again...I just have not experienced any problems with this solution.
Farhad
Thanks for chiming in Farhad. Your experience is such a great resource!
On 8/7/2015 at 7:47 am, Farhad Boltchi (Faculty) said...Damian,
SPEAR is the other half of the Scottsdale Center educational facility. Their curriculum is based on the teachings of Frank Spear, a Prosthodontist, who is hands-down the best educator in dentistry worldwide. Their curriculum is heavy on treatmemt planning and actually understanding why instead of just the how.
Combining that knowlredge with the CEREC digital technology is a "deadly" combination as Ross put it.
Farhad
Hey Damian. I agree with Farhad and others on this site who have recommended the Spear curriculum. As much as CEREC has changed my practice, Frank Spear's teachings have equally done the same. Frank will often say, "you only treat what you see and you only see what you know." This is so true. Spear Education will provide you with valuable knowledge for everyday dentistry so that you can treat every patient comprehensively from a functional and esthetic approach. The course that had the biggest impact on my practice was the Facially Generated Treatment Planning workshop. That would be a great place to start for anyone wanting to get involved with Spear.


On 8/7/2015 at 10:33 am, Farhad Boltchi (Faculty) said...I have to agree with John here.
I have been doing this solution (Maxillary overdentures on free-standing locators) for 15 years now, typically on 4 implants with a couple on 6 implants and a couple on 3 implants.
The only failure I have had was one case where I knowingly pushed the limits and placed 2 X 6mm implants for a locator-supported overdenture....Both implants failed after 2 years.
I know the issue with the concern for this type of treatment comes up again and again...I just have not experienced any problems with this solution.
Farhad
I am happy to hear this from you Farhad. I have been doing this type of prosthesis for 10 years now. Very few failures, Just worn gaskets. For me it beats removing mm of bone the get room for framework, teeth and acrylic. One question. Is there specific benefits to adding 1-2 implants to the anterior area in this case? Misch talks about a possible anterior rock on function that can cause failure of parts and components. I have not experienced much of that. The only issue I have with these cases are relines are a little bit of a pain.
On 8/7/2015 at 8:29 am, Michael Saso said...John,
Very nice end result and nice documentation. Thanks for sharing.
I'm interested in:
1/ how you decided what sites to place the implants
2/ how you feel about maxillary overdentures and long term implant success.
Hey Mike. Thanks for your comments!
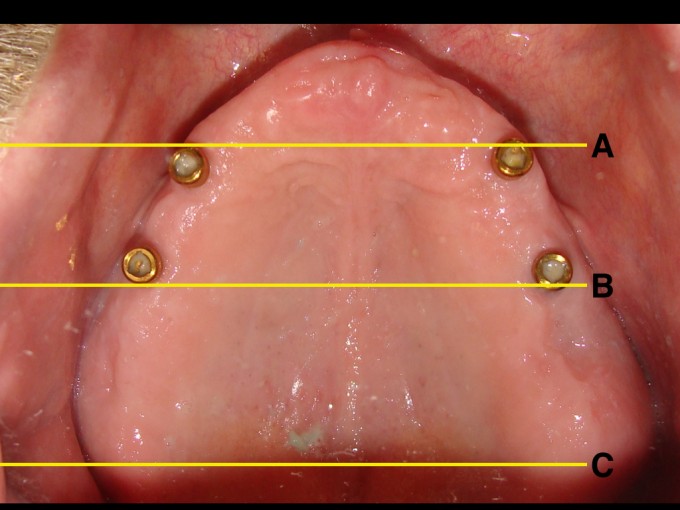
1. These implants are Astra, and I placed them in the areas of #3, #5/6, #11/12, #14, #19, #21, #28 and #30. I decided on these areas based on 1) where the final teeth would be; 2) the thickness of bone; 3) and to avoid ridge augmentation. I have not come across any research that details the position of implants in the anterior. But, the most important aspect of implant placement would be the AP spread which in this case I believe is adequate. See my picture below. The AP spread is determined by the mesial aspect of the most anterior implant (line A) and the distal aspect of the most posterior implant (line B). The AP spread is then calculated to be 1.5-2.5 the distance from line A to B (which is line C). This is a general rule of thumb, and of course, there are other factors to consider as well (occlusal schemes, implant angulation, shape of arch, etc).
2. As for the long term success of the implants and the prosthesis itself, see my previous response to Dan and Rodrigo.

This case here has required some maintainance over the eight years . The patient has all her own lower teeth .She has been edentulous in the max arch for probably 40 years .Originally iliac crest grafts were placed bilaterally and later 6 Straumann implants placed ( all surgery and placement by my OS ) and a metal framed palate less casting made. The implants at the extremities were used as active abutments and the middle ones left a sleepers in case .. ? Eventually the site #6 failed and the middle #4 was brought into function . The patient enjoyed the stability provided and was able to join another choir with the improved retention . The nylon consumables were replaced I think twice overtime and one locator due to wear of the metal cuff edge. About 6 mnths ago on recall the patient lost most retention and there was noted extreme metal wear on the active Locators . I replaced all the active Locators on the 76 yo lady patient and retention and stability was restored . There was some expense to replace the Locators , but the cost was largely absorbed happily by the patient - she was active and infunction again again !
Now , she regrets the loss of the implant in the site approx #6 and asked to see if it could be redone, but there being very little bone remaining after autogratft and the then loss of the implant I referrred her back to my still practising OS .
Whereas I believe she is functioning well a suggestion has beeen made to convert her implants to carry a metal bar of some type - which I am now investigating for her on the suggestion of the OS- we will see where we go however as has been alluded to in this blog " space may prove to be the complication" .
So , my comment here is that extreme wear has occured with metal heads of the Locators requiring replacement, but they have given good service for 8 years and I believe it is not unreasonable to expect replacement after such a period.
BUT , what I want to say to my CEREC.Docs buddies is " it started with a kiss ". Although I didn't do the surgeries , graft and placement when I advised this dear lady she needed a Ceramic crown on a lower premolar I was expecting a rejection and thought she would never do this - she turned to me and said casting her beady eyes in a cold glaze , " Well you had better get on with it then "- I nearly fell off the chair !!! The rest is history and later she accepted the very involved treatment plan - I learnt another lesson about trying to provide the best and today is still a loyal and trusting patient as we now move forward to try and improve her condition to he wish .
these are old photos




On 8/9/2015 at 6:54 am, Clive Dickinson said...
So , my comment here is that extreme wear has occured with metal heads of the Locators requiring replacement, but they have given good service for 8 years and I believe it is not unreasonable to expect replacement after such a period.
Clive mentions the wearing of the Locator abutments ... I used to naively think that the metal should never wear given there are apposed against a nylon bush, but I've found over time that this is definitely wrong, and have had several cases where the replacement of the locator abutment to be the only solution (changing to new stronger /weaker clips did nothing). Another example - I have a chap with locators cast onto the distal of upper canine PFM crowns on both left and right sides! I'm now stuffed - because I can't change them over without making a new crown!
In a current 4 implant over denture case I'm working on the lab is going to make me a milled titanium bar with the Locators screwed into it and I've told the patient that over time they do wear out, but we can just "screw in" a new locator onto the bar.
So for me: telling the patient they may need changing after many years, and that it can be done relatively easily makes it easy for the patient to "swallow" / accept
Ken , Straumann recently ran an evening in Melbourne looking at the topic of overdentures headed up by Dr Anthony Dickinson .
The evening was heavily subscribed and it was an erudite presentation .
He covered the principles of over dentures and followed the guidelines as set out in the ITI texts .
I was able to confirm his findings that wear does occur on the Locator heads at some later stage - and extreme in some cases .
So beware , dont be surprised when you see it . My tip is that the constant removal and replacement asthe patient slides the denture into place there is metal to metal contact against the cuff of the female component , and as the nylon grommets wear there is multiplied metal contact and wear . So perhaps earlier replacement of the grommets may aid in reducing the Locator wear . Perhaps annual replacement may aid the situation .
I will look tomorowto see if I kept the old abutments and show you the wear .
You going to CEREC 30 in Sydney ? - no need for Vegas.
On 8/10/2015 at 6:41 am, Clive Dickinson said.... So perhaps earlier replacement of the grommets may aid in reducing the Locator wear . Perhaps annual replacement may aid the situation . I agree - I always encourage 6-12 month replacement, but most of them just don't come back until their loose!
You going to CEREC 30 in Sydney ? - no need for Vegas. ........ Yes, should be great, I also got a gig to the invite only thing on the Friday
I found a couple of the worn locators - you can see the worn lip 
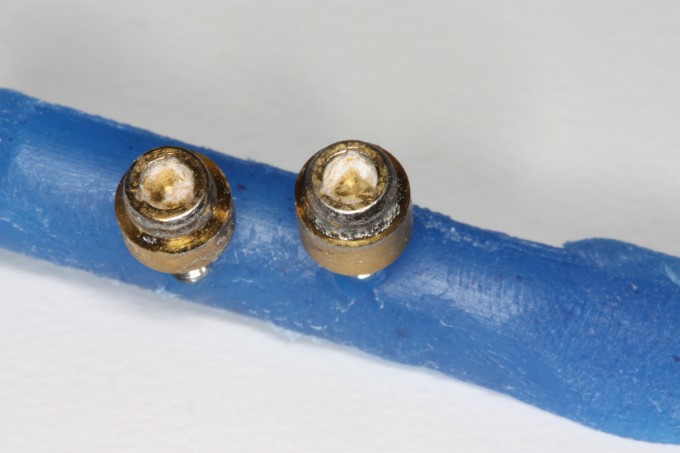
 s of the metal heads.
s of the metal heads.
I think on the centreing of the denture there is metal contact until it glides in.
See ya in Sydney .