Pre-Extraction Bone Grafting

The treatment of the hopeless teeth in the esthetic zone remains very challenging due to the pre-existing anatomical limitations. Out of the various available treatment options one strategy which can be employed is that of pre-extraction bone grafting illustrated by the following case report.
A healthy female patient presented with a maxillary left central incisor with advanced external resorption and a very deficient alveolar ridge anatomy (Figures 1-3). Although the tooth was deemed to have a hopeless prognosis it was asymptomatic. A decision was therefore made to perform a minimally invasive pre-extraction bone grafting procedure via a lateral tunneling approach using a cortical mineralized/demineralized blend allograft (Maxxeus Cortical Min/Demin Blend Allograft) mixed with platelet-Rich Fibrin and overlayered with a long-resorbing highly cross-linked collagen membrane (Ossix Volumax) (Figure 4). Six months after the bone grafting procedure a CBCT scan and a CEREC optical impression scan were obtained and the corresponding digital data were uploaded to the Dentsply Sirona Azento portal to obtain a guided implant surgery treatment plan. The post bone grafting CBCT scan revealed a radiographically well consolidated bone graft and adequate augmentation of the previously deficient alveolar ridge (Figure 5). An implant treatment plan was devised through the Dentsply Sirona Azento workflow (Figure 6) and the Azento surgical guide was then utilized to place an immediate implant (Astra EV 3.6S X 13mm implant) at the time of tooth extraction in a minimally invasive flapless approach (Figure 7). The post implant placement CBCT scan revealed an implant accurately placed within the augmented alveolar ridge in accordance with the guided implant surgery plan (Figure 8).

Figure 1: Pre-operative clinical presentation of tooth #9

Figure 2: Pre-operative periapical radiograph of tooth #9 with external resorptive lesion

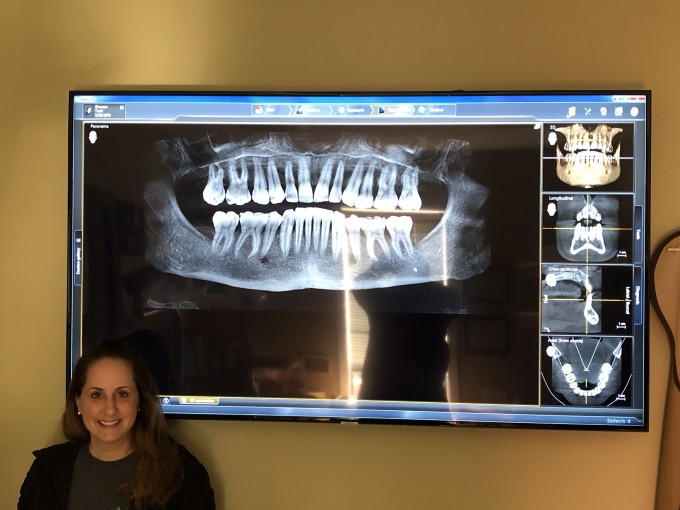
Figure 3: Pre-operative CBCT scan of tooth #9 with deficient ridge anatomy

Figure 4: Pre-extraction bone grafting via lateral tunneling approach

Figure 5: Six months post bone grafting CBCT scan of tooth #9

Figure 6: Dentsply Sirona Azento implant treatment plan site #9

Figure 7: Occlusal view of immediate implant placement site #9

Figure 8: Post implant placement CBCT scan site #9
The pre-extraction minimally invasive bone grafting technique employed in this case allowed the augmentation of the deficient alveolar ridge prior to extraction of the hopeless but asymptomatic tooth. This strategy can be used in certain cases to allow the patient to maintain the natural tooth with a guarded or hopeless prognosis while the bone graft is healing. Implant placement can then follow with a minimally invasive immediate implant placement technique. A major advantage of this workflow is that it avoids the need for the oftentimes challenging provisionalization during the prolonged period of bone graft healing. Furthermore, this workflow results in minimal disruption of the delicate gingival architecture in the esthetic zone thereby significantly enhancing the final esthetic outcome.
Hi Todd,
I will not do a PET/Socket Shield in a resorption case (such as the above case) as I am not quite sure if the residual root fragment will be prone to further resorption.
Otherwise this case could have been handled with PET technique at the second stage but not at the first stage as there was not enough bone apical to the root. So even with PET the pre-extraction bone grafting would have been handled the same way.
Farhad

Farhad Are you able to get primary closure of the incision? If so, do you do this by stretching the periosteum? Thanks -
TT


On 4/27/2021 at 9:53 am, Anthony Tisoncik said...Farhad Are you able to get primary closure of the incision? If so, do you do this by stretching the periosteum? Thanks -
TT
Tony,
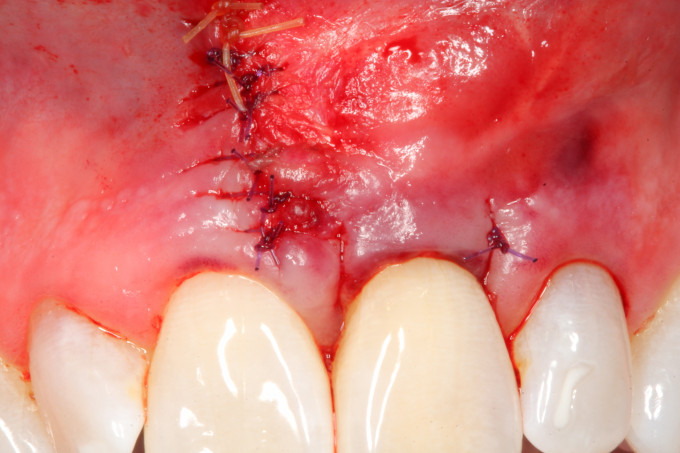
Primary closure of that lateral tunnel access is usually pretty easy as the incision in mostly in mucosa but if needed you can stretch the site a little....Most of the time that is not necessary though. Below is the sutured picture of this case.
Farhad
On 4/27/2021 at 10:27 am, Michael Mingle said...Farhad, is that a xenograft with volumax or allograft with volumax?
Mike,
This is pure Allograft with Ossix Volumax as I want all of that bone to turn over into bone. Theoretically one could place an outer layer of xenograft as protection but technically that is impossible to accomplish through that tunnel access.
However, Ernesto Lee who teaches the SMART technique uses pure xenograft mixed with PDGF and shows beautiful results as well so a membrane may or may not be necessary. I am still playing with the technique as to see what works best in my hands so I am a little more conservative at this time.
Farhad

On 5/6/2021 at 9:22 am, David Sorensen said...Do you graft the gap after you place an immediate implant?
David
Yes David. At the second stage it is just like any other immediate implant placement.
Farhad