Any Feedback on this prep/onlay vs full crown or other suggestions?

Hey any West coasters, late night people or early risers... I had meant to get this case posted earlier in the day or week, but hadn't. I'm presenting an onlay case to some other docs and wondered if anyone out there had thoughts on the prep, the design and pros/cons of the way I treated the tooth. Note - I am pretty much an A1 block guy, so don't harass me too much about the shade of the block! I have been doing these onlays since 2002 with very high success, but am training some other docs and want to see how many in the community would do an onlay type prep as I did here, or something LESS invasive, like a composite, or more of a full coverage crown.
Initial presentation: 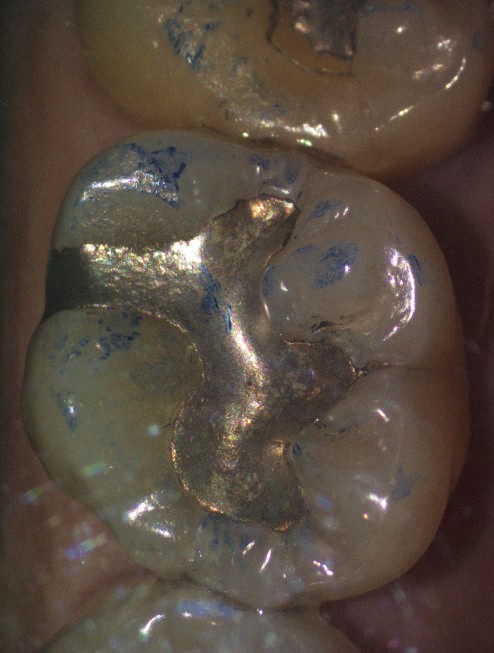
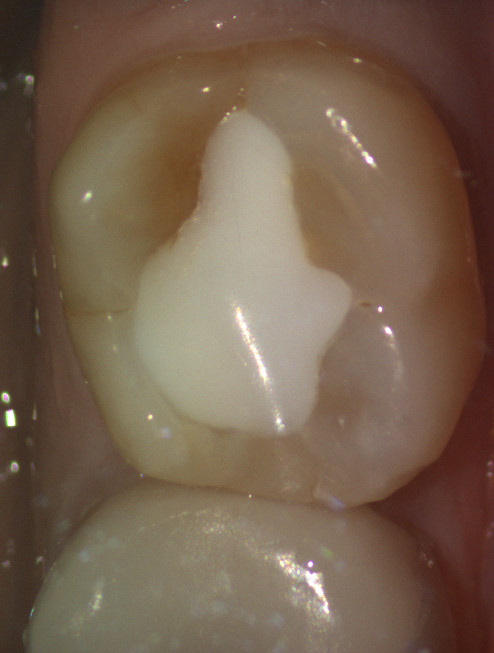
Removed the Amalgam and recognized the mesial crack was extending onto the pulpal floor: 
After shaping around the mesial fracture, noted the pulpal fracture on the DB cusp, but since the crack was on the floor only, decided not to hood the entire molar: 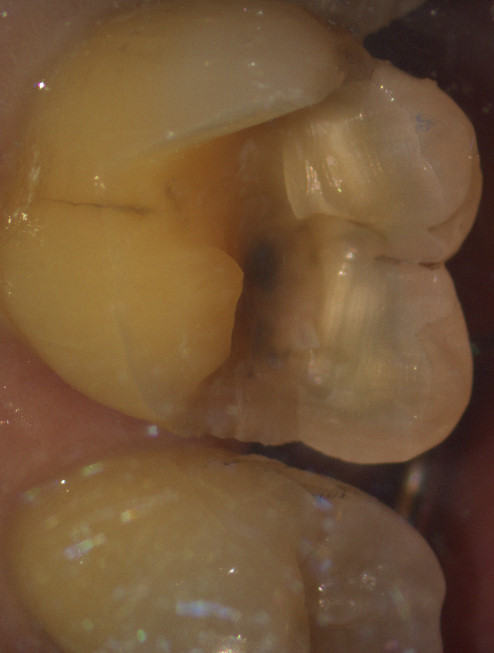
THoughts on this? Better to hood the entire buccal?
After shaping down, preparing with very slow speeds and finishing the margin, didn't like the 2nd dentin and the high MB pulp horn: 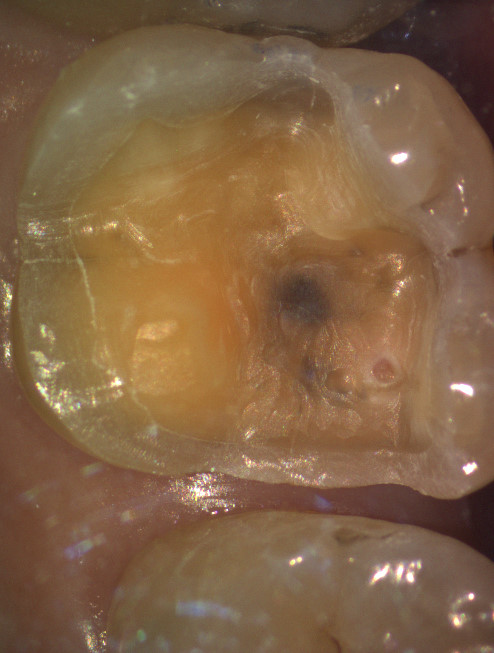
So placed some CaOH: 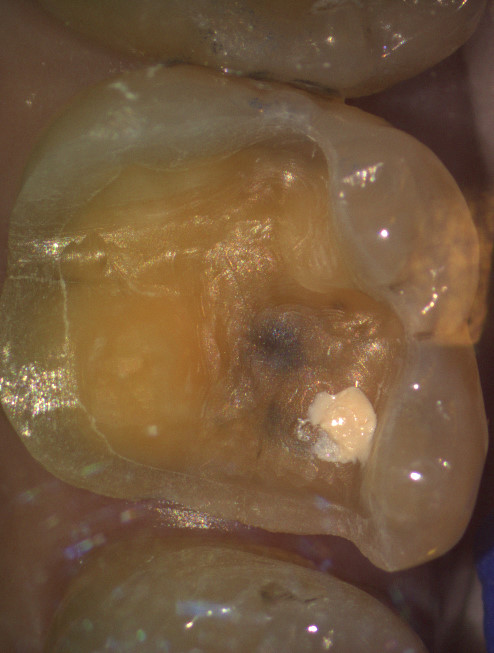
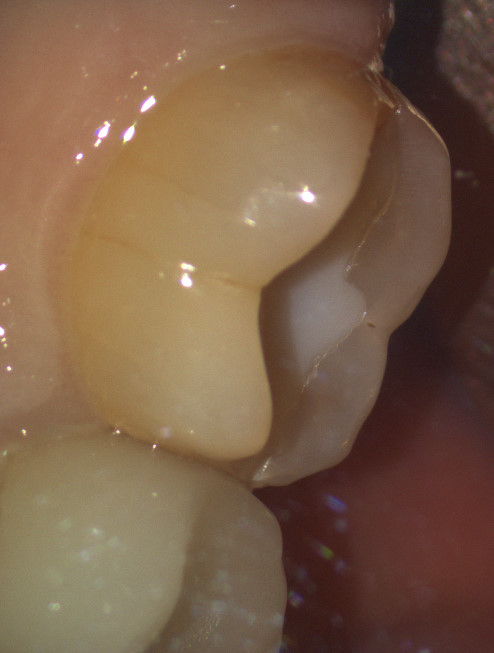
And after cementing and comparing the final occlusion, thought we looked pretty good on this restoration: 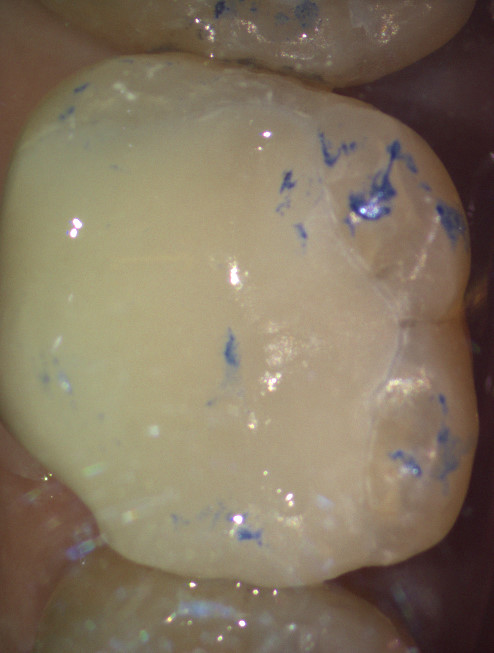
I have a tendancy on molars that have had heavy occlusion with large amalgams to reduce the overall bite so from the initial biocopy, you can see the reduction of the heavy bite and I'm wondering how others would have managed this case. Original biocopy:  Adjusted occlusion:
Adjusted occlusion: 
Thanks for any thoughts! Curious how many would have just done a composite here... how many like the onlay.... and how many think this should have been full coverage- or MORE coverage than what I did here. Appreciate the feedback!
Steve

Personally, what I would have done would've been a crown. Initial presentation looked like a good onlay case to me as well, but when you began running into the cracks (especially under the DB cusp, I changed my mind to a full coverage crown. Was there decay in the mesial side of the tooth? If not, I believe that doing the crown after the amalgam was removed and the cracks noted, would have kept you from approximating the pulp horns as you did, and would've preserved more coronal tooth structure to retain the crown. Just my 2 cents.
Paul
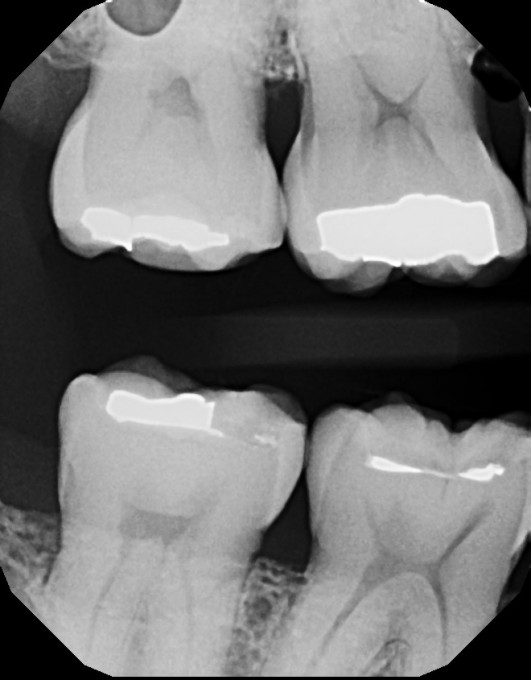
No real decay, just a really high pulp horn (I think has since receded and this is more 2nd dentin from the receded horn). I didn't really remove much/any after removing the enamel. Here is the pre-op film.
Thanks for the thought... hoping to get a lot of thoughts. I have not personally seen onlays that I've done like this, have the other cusps fracture off over long periods of time when seeing these fracture lines on the pulp, but they still don't make me happy to see them!

I typically leave the tooth alone too in these situations. Let patients know about the expansion/contraction, etc and let them decide- most opt to do nothing. I also tell them that odds are fairly high, that the treatment when they have an issue with this tooth would be the same to prevent anything in the first place- a crown.
This is a great case to show though. Lots of differing view points regarding treatment. Which one is best? Im not sure there is an answer.

I grade teeth like this so i can see 'change over time'. grade 1 2 or 3. 1 is 'see cracks in enamel around amalgam/comp'. 1 doesn't mean anything other than we can visually see them. usually 1 has no symptoms. grade 2 is a slight greying or the crack. usually there is occlusal breakdown of the restoration along w grade 2. sometimes there are symptoms but intermittent. then grade 3 - much darker crack and more frequent symptoms. We have created custom codes in detrix to track this. and from that information we can see how things change over time. it's not perfect but nor is the decision process that is 'waiting for pt to have worse symptoms'. at least this way the patient has the information, knows things are SLOWLY worsening and that in time they will decide on a course of action and it's not a surprise.
So, that being said, this tooth would be a grade 1 tooth, maybe a grade 2 tooth (on mesial looks grey but maybe pic is different). if the patient had occasional symptoms i would assign them grade 2. with the high pulp horn i would say that 'waiting for this tooth to worsen is probably not a great idea. fractures need to be contained, that's what crowns do. onlay might work but it depends on the cracks under the filling. in either case they have a risk of needing a future RCT but w a crown their chance of pain on biting from incomplete fractures within the tooth are greatly reduced/minimized.
Once the amalgam removed, it would be a clear crown to me. i'm out of network and my onlay changes and crown charges are similar as it's similar work. But that's how i would have talked it through and the most likely result for this pt would be an emax crown or zirconia (depends on pt age, esthetic needs, their expectations regarding future patching vs recrown, etc)
hope that helps. this system has worked well for us.
Bill Argersinger

Let me start off with the fact that I dislike partial coverage restorations. I've been around long enough to see most of those fail to either proximal decay on an unrestored surface or fractures within the non-restored cusps.
My goto restoration is the full coverage onlay. I have been doing them since 1996, first with a lab, then with Cerec since 1999. They are great restorations. My decision point in fill or onlay is the presentation upon transillumination. While the mesial crack would not have been enough to get me to even think about an indirect restoration, the other crack would have.
Brian,
do you break contact on the mesial and distal or do you just prep past the cracks? i have always wondered how cerec handles the M and D onlay preps if you don't break contact.
Bill
I always break contact. Meissinger 2.0mm bur to set my mark on cusp removal and depth of central groove area. Drop boxes, smoothen everything and image.
I agree with what's been said above about the range of txmt plans (far from surprised though). Several "I'd do nothing" and several full crown concepts... Pretty much what I expected, but I'd love to continue hearing peoples feedback and experiences. Honestly, I've been doing mostly onlay restorations since 2002 when I came out of school. Initially 2D cerecs on the old, OLD camera and mill unit, up to a red cam, up to a blue cam, and now omni. I haven't done a "Traditional" crown prep in a long time with the exception of removing an old PFM and just biocopying into a new crown. When I have felt the cracks are pervasive enough, I still lean strongly towards the "cronlay" approach with VERY supragingival margins on that thick band of enamel vs that of a traditional crown prep. Good enamel bonded with a full resin cement trumps all mechanical retention in my mind (I removed an onlay from my partner from 2001 a few weeks ago and every last little square millimeter of Cerec was FIRMLY adhered to the tooth).
I can relate to the comments about leaving the marginal ridges unprepped as I did on the distal here b/c I have long known the preps that I do, do not fit traditional design concepts. I often leave the marginal ridges like these (probably have thousands of restorations like this out there) and have only seen a very small % fracture over years. Because they continue to be successful year over year, I haven't changed my prep designs!
A big reason I posted this was to see the range of txmt plans and get input because some of my local colleagues and I were having a discussion on how to txmt plan these types of teeth and I wanted to hear some CD opinions before that meeting. So please, keep the perspectives coming. I don't know that I'd recommend someone prep how I did, it has just been working for me for 15 years now. I know many would be very surprised to see the marginal ridges we have kept or even to the point about not breaking contact- traditionally we almost always break contact. However, I routinely leave the prep ~2-2.5mm below the marginal ridge or slightly more and have the contact remain in tact. Cementing can be the challenge, but I've used a technique for 5-10 years now of simply inserting a very thin segment of tofflemire band in the interproximal and placing a wedge below the contact point. It works very well, but is a technique we've developed over the years. If done properly, the onlay seats to a full seat and it allows us to keep the prep very conservative.
These types of preps and techniques take a lot of effort, and cementing can really be a pain, so again, I'm not sure I'd recommend them, but they do work. I have only seen issues of recurrent Cx in highly caries risk patients. For the gross majority, if they don't have hypomin at 40 or 50 years old, and the dentin and enamel look good on a film, I don't see why they would develop interproximal caries now that the tooth has an onlay.
That is just my personal experience. I always strive for 2+mm of porcelain, keep the preps super smooth, do a total etch and cementation with Variolink (I have seen and heard of a lot more failures with multilink or other self-etching cement systems), maintain excellent isolation throughout, and then manage the biting forces in CO and excursive. With those basic principles, our failure rate has been extremely low, but I recognize that more and moreso, cuspal coverage has been the norm. Frankly in the past with the blue cam we were even more conservative in our prep design than now, but with the omni still struggling with onlays and also trying to think through a lens of 20 to 30 years, vs 15, I'm covering more cusps now than I had in the past, but we still (like this case) leave many cusps uncovered.
Thanks again to all who have chimed in already, and I'd love to hear even more opinions. I routinely hear in Scottsdale that docs are nervous of these onlay preps, so would love to hear more peoples experiences with them and if they've seen failures over time.
Steve

I think this is a great topic of discussion and if you ask 20 dentists, you are going to get 40 treatment plans. My personal opinion is considering the size of the amalgam that was present, and assuming lack of symptoms, I would have done nothing and if the patient wanted to replace the amagam for esthetic reasons I would have done an inlay in this prep:

Obviously Im coming from a perspective of a monday morning quarterback - I dont know the patients desires or have not done a clinical examination -but this is how I would proceed with the case.
One thing you learn when you have been around for awhile is how tough teeth really are, and also how fragile they become when too much dentistry is done on them. We all see the 80-something patient with huge amalgams that have left the tooth and restoration working fine. The dental school mentality of achieving an ideal has caused more teeth to be prepared than necessary over the years. When you get a chance to see your own work after 30 years or more, one starts to realize that maybe a less aggressive choice of restoration or no restoration at all would have served the patient better.
I'm not ripping on the OP at all, but philosophically, we have all developed a sense of when to attack. Younger docs are still influenced by their school and/or choice of CE, and older docs by experience.

I would have referred to therapist to undertake direct composite or equia forte restoration as minimal intervention if this was my tooth!
Yeah, thanks for that Sam. Patient had asked about getting rid of metal and wanted upgrades... The patient also was the type to select "best care" vs "the cheapest replacement". I did 6 teeth that day. 5 composites and this onlay. Did the onlay over composite mostly b/c of the mesial Fx line and I figured once I got into the amalgram undercuts, I'd be dealing with a lot of tooth structure loss, and frankly, I wouldn't personally want a composite that large. I did decide to leave the distal even though it had some "crazy lines" (of 5 colleagues 2 said they'd have prepped the distal, 2 went full crown and the other was a no comment- I'm not sure any of them were wrong to your point Sam!). No one seemed to be a of a STRONG opinion and one said "this is the type of tooth I'm just not sure what to do". I do think many of these we are often surprised once we take the amalgams out, sometimes at the amount of decay under... sometimes the amount of proximal fracture lines, or pulpal fracture lines.
I phrased it this way during our discussion... my txmt plan probably would have depended on how many fractured teeth I saw in the previous 2 weeks!
I'll be preparing for one of our meetings is hopefully 20 or so cases of "pre-op" teeth... then do the same thing where we discuss our txmt plan and then go through the preps. I expect to see a wide range of txmt plans, but I think it's good for us all to discuss.
Here's another case that I'm sure will drive some crazy b/c I left the buccal cusps in tact, but on initial exam it had the typical distal crack off #18 and the lingual to match, and recurrent caries on the mesial under the old composite:
Very obvious on initial preparation how severe that distal crack is/was:

Then after removal of the old mesial composite, doing caries removal we ended up roughly here (don't know if I got a FINAL prep photo, but this was close to finished for me). It's hard to see on the cerec cam images (sorry, too lazy- and probably already behind with patients!- to go get my mirrors, SLR cam, and take a GOOD photo!) but if you take my word for it, the distal crack there runs (like it typically does) from the distal, about mid tooth and then curves around to join that lingual fracture line.

Now, we all see 2nd molars every day that have this abrasive "V"'d out pattern on the distal (side note: why do the lowers always V out, and the upper palatal cusp maintain their enamel? That's always confused me why the lower tooth "loses" in what seems to be a 50:50 battle)... often with the distal crack... often with the lingual crack. Most are asymptomatic, but I personally don't feel that means that they aren't in trouble! The issue I always have in txmt planning is you really don't know how bad those cracks are until you get the restorations out! We leave the majority of these "crazy lines"/fractures as non-txmt planned in our practice, but the longer I get into dentistry, the more I guess I'm sensitive to patients fracturing their teeth in some catastrophic way- "why didn't we treat this earlier, doc" (yeah... why didn't we? Oh, because insurance wouldn't have approved it)!
I'm a strong believer that MANY of the endos out there that fracture after the endo and the crown (maybe 1 year, maybe 10 years, but same principle) is b/c by the time we treat these cracks, probably many of them are already into the pulp, and maybe well onto the root structure. Ever try pursuing these cracks until they "end" - e.g. to the eye with loupes? I usually stop b/c you start getting pretty sub-G, and you are losing your enamel the further you go apically. I usually try to find that "healthy balance" where the crack seems small enough, but I'm trying to save enough enamel to get good bond strength of the restoration. I hope others can relate... So, I guess my question is - have we already waited too long at that point?
So, on that tooth.. we do our onlay or crown... 5 years later the tooth needs endo, and 5 years after that it fails due to root fracture. Is this one of those "RCT teeth fracture more often"? Or are RC teeth a biased pool of teeth that already have these deep cracks that end up getting endo? That's my personal bias, that endo teeth aren't more likely to fracture, but that teeth that have endo, have (by the time they get their endo) ALREADY undergone substantial structural loss, and it's just a matter of time (e.g. crack propogation, albeit slower now that the crown is on) before the crack down the root leads to complete failure. Of course, some never do... but plenty DO! What if we had treated the tooth 5 years prior? Would we have avoided the RCT... the crown and the eventual implant? Which is more conservative of an approach in the long run? Are we just avoiding the uncomfortable conversation with the patient about treating a non-symptomatic tooth ("but it doesn't hurt doc")?
Anyways, that's been my working perspective, and again, the longer I'm out here doing this, the more sensitive I am to being a bit more proactive with when to prep- yet conservative in prep, so that in the long run, maybe we avoid some RCT, Crown, EXTs.
So, sorry to ramble on, but I've wondered if others are experiencing the same things in their practices b/c I know we shouldn't treat every crazy line, but I also think especially on 2nd molars - if we're too slow to treat, we may be causing the patient more long term issues and greater risk of future root fracture.

Great topic. I tend to agree with Brian based on my long term experience with partial coverage. I would have likely left this tooth alone. However, if the patient wanted treatment I would have started out with a plan for direct composite. Upon seeing those cracks, I would have done an onlay.

I would leave that tooth alone or place composite filling. I think the treatment was too agressive. This is just my opinion. My partial restoration have a good success. Gregory