 Darin O'Bryan, D.D.S.
Darin O'Bryan, D.D.S. This is a case that I have been meaning to post for a while. It really shows the importance of proper surgical training to make sure that you have a good feel for what drilling in to bone feels like and also when something just doesn't feel correct.
The patient in this case is an elderly gentleman that was edentulous posterior to the bidcuspids. Due to a nerve injury suffered during military service he is incapable of having anything past the bicuspid area. He had two existing bridges. One of which was the area of concern. There was recurrent caries under both abutments 5 and 8 respectively.

The plan was to remove 5 and 8 with concurrent placement of implants in the area of 5,6 and 8.

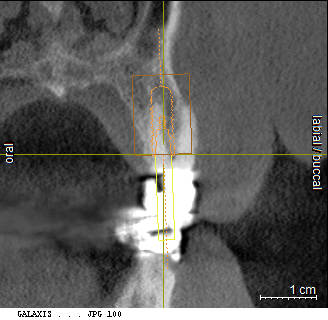
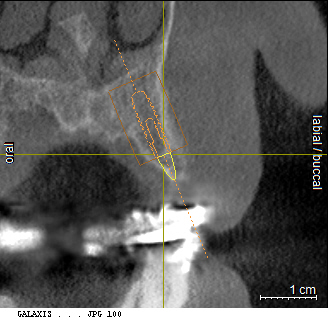
As you can see there is not a lot of wiggle room for #6 implant. I got a guide done by codiagnositcs. The reason I used them was I had already gotten the CT scan and didn't have the bite plate at the time. I didn't want to rescan the patient so with this method I was able to get a guide fabricated without having to rescan. The stone model was digitized and used to fabricate the guide. I also wanted to try out other options that are available to use. So I extracted the teeth a traumatically. Now as can be seen on the CT cross section of #8 there was not a lot of buccal bone. After extraction and inspection of the extraction sites is when things didn't feel right. I had planned on flapping to help build up the area of 6 but upon inspection of 8 the buccal wall felt "weak".
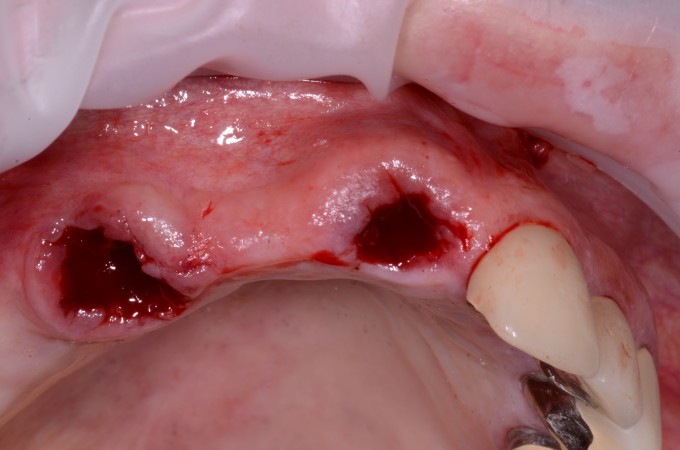
So I flapped it and with just the action of gentle reflection of the facial tissue the buccal plate at the coronal aspect peeled away with the tissue.
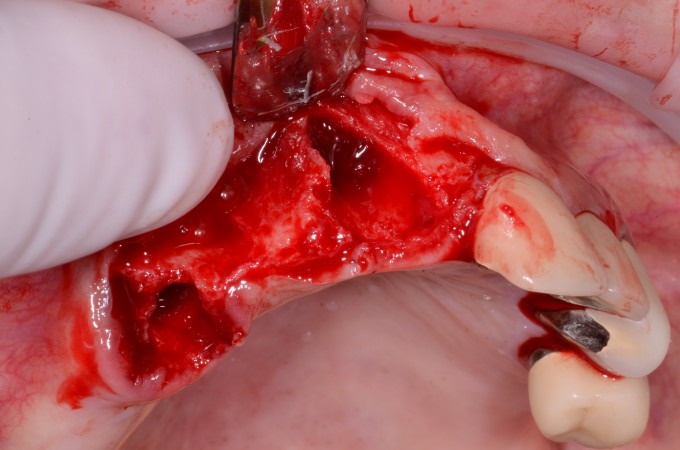
So now I am definitely having to graft. I verified the fit of the guide.
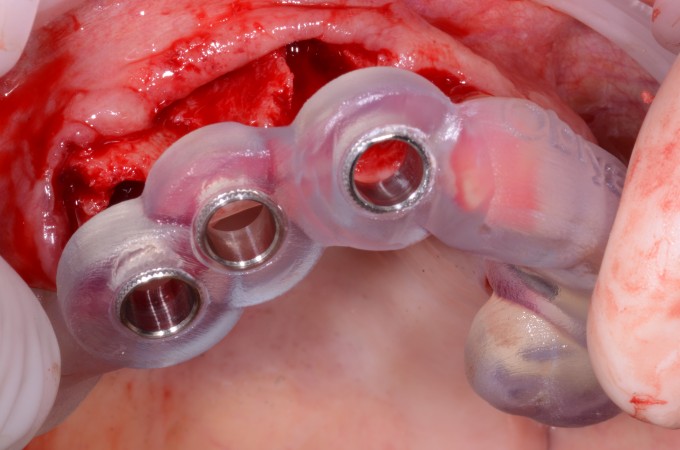
I then went ahead and started the osteotomies for the three locations. The two in the extraction sites went very smooth. The one for #6 didn't feel right when I drilled into the area. So I removed the guide and looked at where the osteotomy was. Low and behold it was lingual to the designed location.
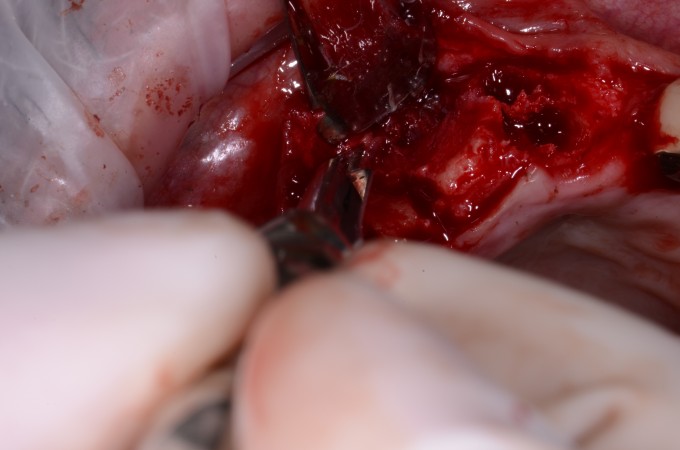
What appeared to have happened is with no distal support for the guide the drill deflected off the hard ridge and gained purchase lingual into the palatal bone. This is where having a good grasp of surgery helped. The feel of the drilling into the bone did not feel right given the density of the ridge and then of course when probing the site it really didn't feel right. If this case had been done flapless it would have been very likely to place the implant and get good stability, however the implant would have only had the apical third completely in bone the coronal two thirds would only have had bone on the facial, mesial and distal. Just enough to integrate but not enough for long term success. I tried to free hand the osteotomy but with the damage to the lingual aspect all I got was a nice through and through defect to repair.
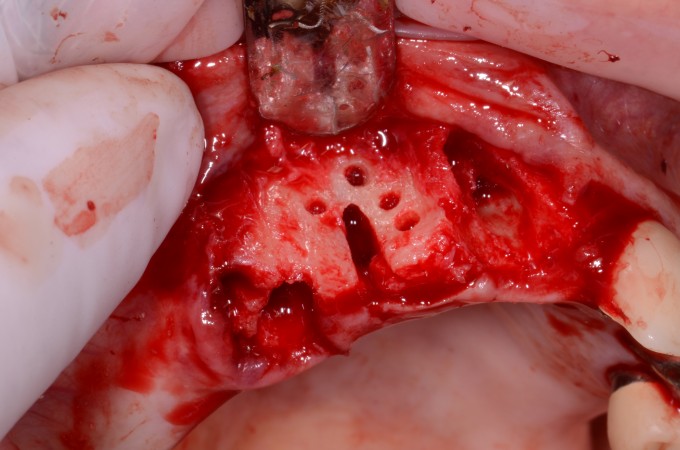
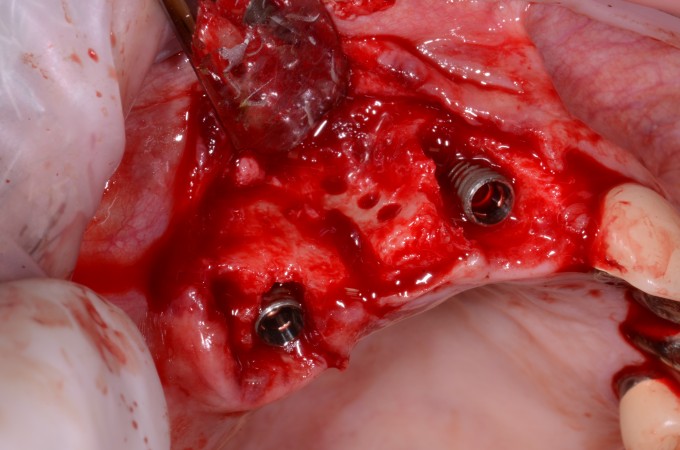
I went ahead and punched a few holes in the buccal plate to allow for medullary bleeding. I then placed the implants in the extraction sites.

So now the reconstruction of the facial area needed to happen. First we mix some a-PRF with cortical cancellous bone and Bioss. 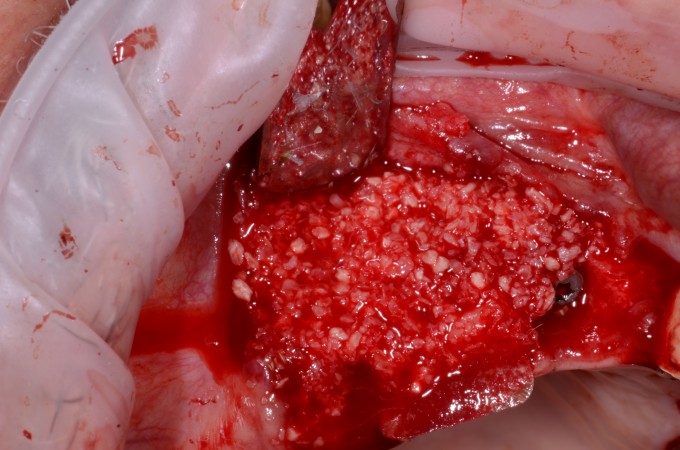
Then our membranes are placed. This is the sandwich technique that Farhad talks about.
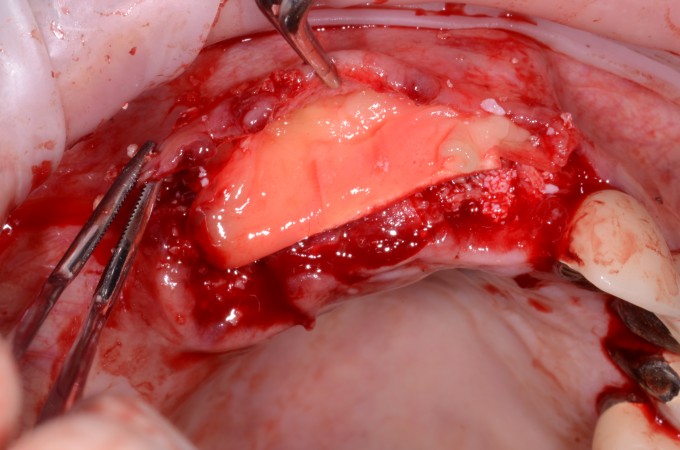
Then we suture it closed and allow it to heal. I buried the implants to after it healed we had to uncover and let the healing abutments settle in. Here is the site after healing. Note the thickness of the buccal area after grafting.
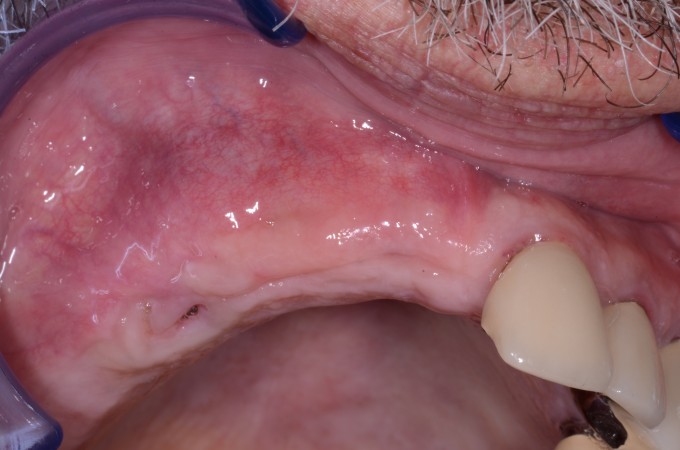

Now we just need to temporize while the lateral wall grafting continues to settle in and stabilize. I want to give it a good 6 months before going back in to place the implant in the site of #6. So once the sites are uncovered we reline a shell temporary and recontour it to give good tissue and papillae support.


Now we wait. Once the bone has healed I will get a new scan and fabricate a guide to place the implant in the location of #6. With good stability we will reline the temp at the day of surgery. Then the restoration will happen.
The big take away from this is while guided surgery is definitely a huge benefit for us and our patients we as surgeons still need to have good surgical knowledge to be able to evaluate what is happening during surgery to make sure it is going as planned. And if not how to handle the complications that can arise.