SLEEP THERAPY Article
Understanding the Hypoxic Burden Index: The Metric Every Dental Sleep Medicine Provider Needs to Know
Dr. Jonathan Ford
CDOCS Faculty

When any dentist begins treating sleep apnea patients with mandibular advancement devices (MADs), the biggest clinical concern I always hear from colleagues was, “What about the bite change? What happens if the patient’s occlusion changes?”
It’s a valid concern. But here’s the truth: bite changes don’t have to be unpredictable—and they don’t have to be deal-breakers.
First, I want to put things in perspective. All medical treatments come with side effects. Just listen to any pharmaceutical commercial. Sleep apnea patients aren’t breathing well. They are suffocating every night while they sleep. In my opinion, a consistent and constant lack of oxygen every night trumps a potential occlusal change. If we truly and honestly want to rank the severity of side effects, lack of oxygen is the most severe. We need oxygen to survive every 30 seconds. As dental providers, we need to mitigate those dental side effects for our patients, and we can. Let’s review through how dentists can do that.
To have success with MADs, it comes down to creating a comfortable appliance that patient will wear and be compliant with. We need to select the right appliance for the right patient, managing expectations, while simultaneously, mitigating forces. Here are a few principles that guide how I approach this in my practice.
1. Appliance Design Can Dictate Tooth Movement
Every appliance has a personality. Some exert more pressure on anterior teeth, some on posteriors, some on both. If you’re not taking this into account during selection, you’re inviting unintentional movement like decreases in overjet, or open contacts. I lean toward appliances that minimize forces on the anterior teeth and put forces on stronger teeth. What teeth are the strongest and what teeth will resist movement? I go back to what teeth can support bridges and what teeth typically cannot.
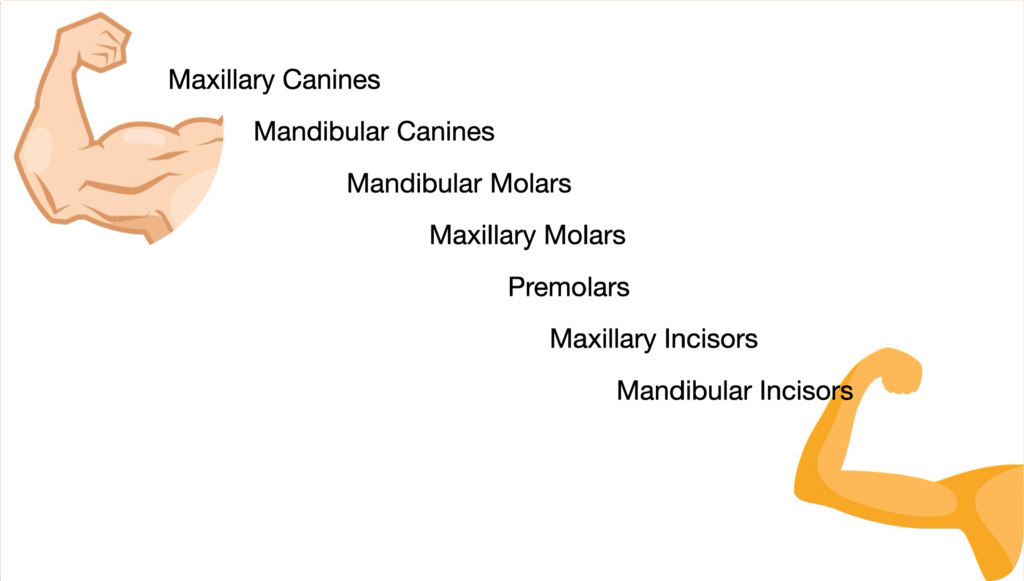
Canine and molars are the strongest teeth, so let’s select a mandibular appliance that uses those teeth as the foundation for support.
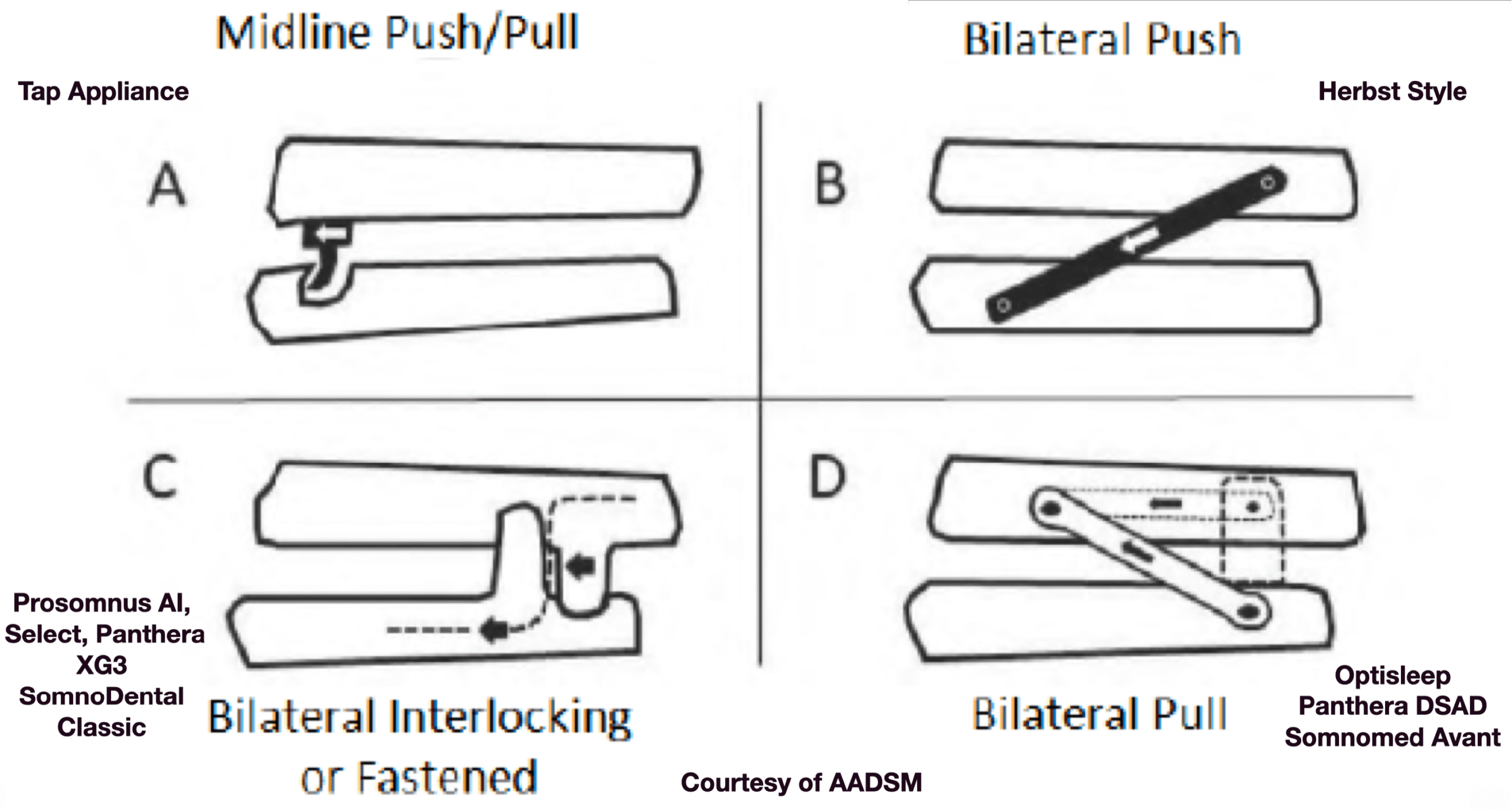
I also look at orthodontists. When orthodontists do Class II corrections and use elastics, what teeth do they use for anchorage? Typically, maxillary canine and mandibular molars. If orthodontists have been doing this for decades, I typically like to mimic their designs and use MAD that use maxillary canines and mandibular molars for anchorage. These appliances are called bilateral traction/pull devices. Examples are Panthera DSAD or Optisplint by Sicat.
2. Setting an initial start position and titrate conservatively
Each patient will have their own unique range of motion as their mandible moves in an anterior posterior direction. The farther the patient is titrated anteriorly, the more pressure get applied the masticatory apparatus. More force potentially means more tooth movement. I typically set the initial start position at 50% of the patient’s total range of motion. If the patient is responding to treatment at their initial start position, we can achieve optimal results with limited forces. If the sleep tests still show suboptimal results, we can begin to titrate or move the appliance in an anterior position. Monitor closely, and titrate if needed, but follow up with sleep test to show objectively, the patient is breathing and sleeping better.
3. Let Patients in on the Conversation
The reality is that most patients won’t care about minor bite changes—as long as they understand the benefits and are brought into the decision-making process. I’m upfront: “There may be changes, but they’ll likely be manageable, and here’s how we’ll track them. There are also additional steps we can take to mitigate bite changes. They are morning occlusal devices and Essix retainers, but I need you to wear them every day!”
4. Track, Document, Adjust
Use digital scans and regular documentation to monitor shifts. It’s easy to get clinical tunnel vision—digital records help you spot trends and adapt early. The digital scan also gives your lab the ability to make a better fit, more accurate, and therefore more tolerable appliance. This leads to better acceptance, higher wear time, and better clinical outcomes.


Conclusion
There’s no one-size-fits-all solution. But with thoughtful selection and a clear protocol, you can prevent surprises and build patient trust—while delivering better airway health that leads to better overall health.
Related CDOCS Hands-On Workshops
Implementing Cone Beam for Practical Utilization (CB110)
Get comfortable with cone beam technology through hands-on training in CBCT hardware operation, full volume review, and Sidexis and Sicat software suites, including introductions to CAD/CAM integration, airway analysis, and implant and endodontic applications to unlock your system’s full potential.

Integrating Dental Sleep Medicine for Patient Care & Practice Growth (CB150)
Expand your practice into dental sleep medicine with training in obstructive sleep apnea screening, home sleep testing, oral appliance selection and fabrication, complication management, medical billing, and strategies for building lasting relationships with referring physicians.