IMPLANT Article
Connective Tissue Grafting for Root Coverage Anterior Mandible
Dr. Farhad Boltchi
CDOCS Faculty

Challenging Root Coverage in the Anterior Mandible: Autogenous CTG with Modified Tunneling Technique
Root coverage in the anterior mandible remains one of the more complex procedures in periodontal plastic surgery. The thin biotype, limited keratinized tissue, muscle pull, and anatomical constraints in this region often make achieving predictable, esthetic, and long-term root coverage difficult. However, with advanced techniques and refined instrumentation, successful outcomes are increasingly attainable.
Below is a clinical case example illustrating the use of an autogenous connective tissue graft (CTG) combined with a modified tunneling approach to achieve root coverage in the anterior mandible.
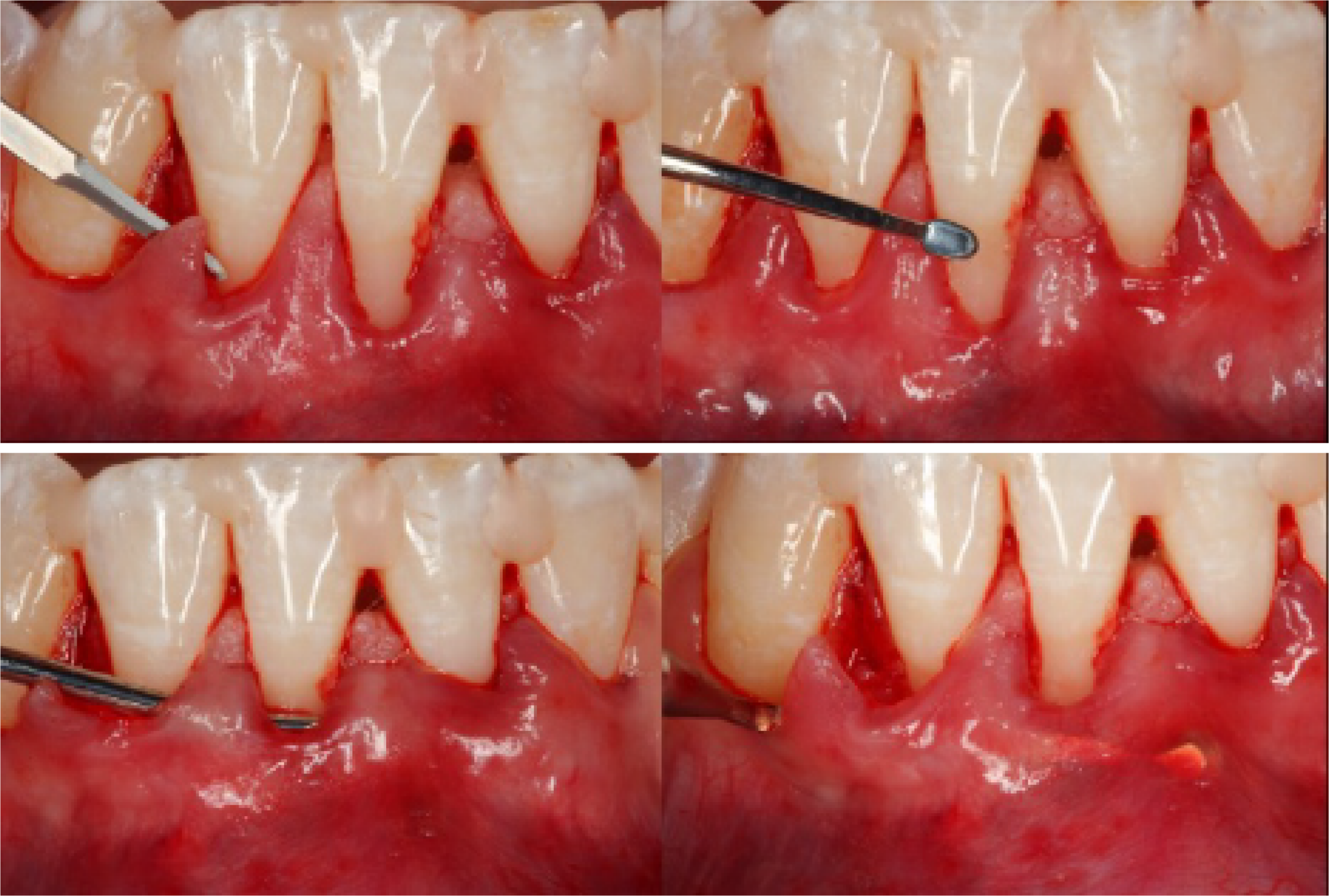
Technique Overview: Tunneling with Partial-Thickness Papillary Access
The selected surgical approach involved tunneling with partial-thickness dissection, carefully preserving the papillae. This method allows for atraumatic access while maintaining vascular integrity—critical for graft survival in the anterior mandible. The use of partial-thickness dissection minimizes trauma and reduces the risk of flap perforation, especially important in areas with minimal tissue thickness.
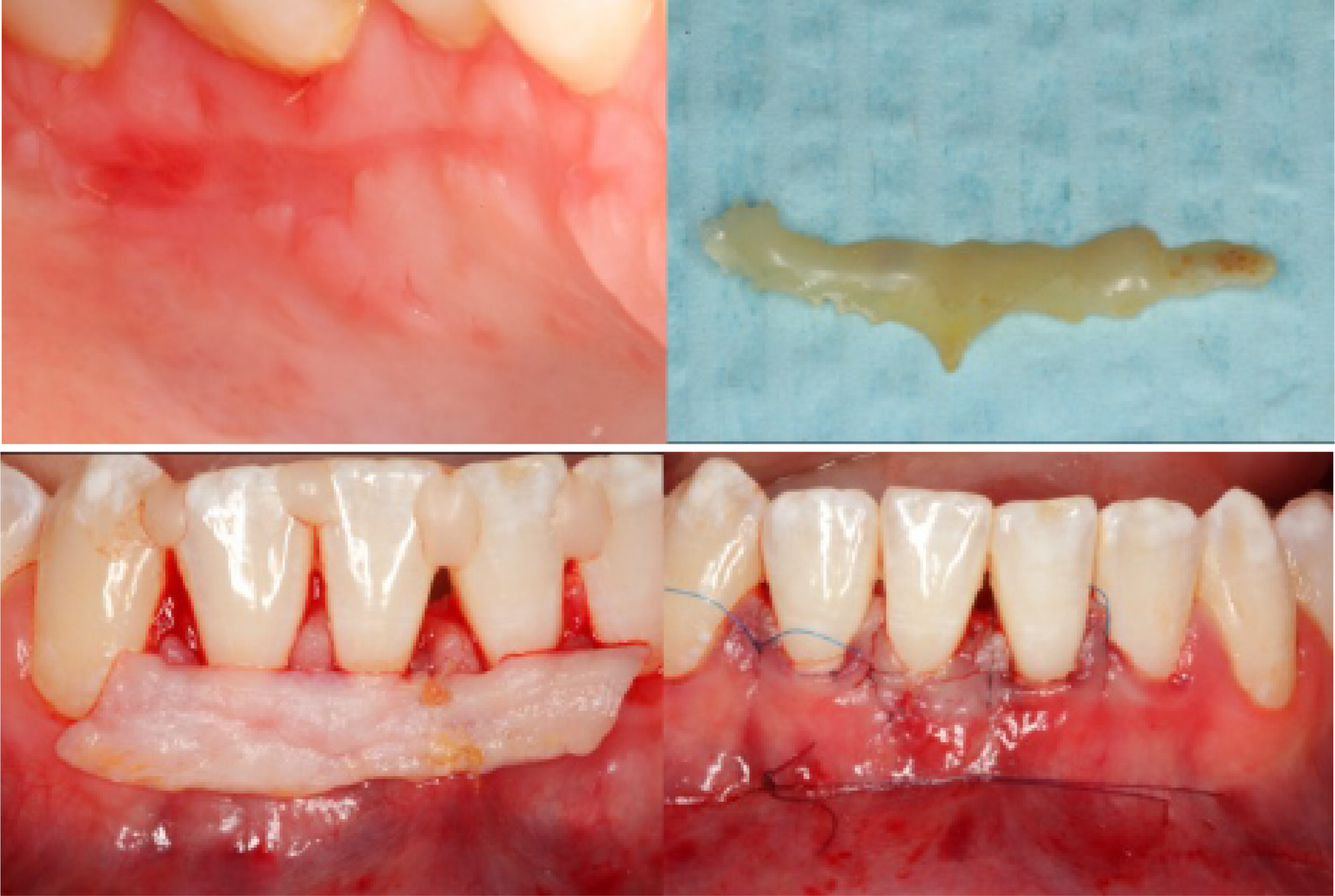
Graft Harvesting: Lateral Palate with 2mm Double-Blade Technique
The connective tissue graft was harvested from the lateral palate using a 2mm double-blade technique, allowing precise and consistent tissue thickness. After harvesting, the graft was de-epithelialized to promote integration and avoid epithelial island formation. Hemostasis and patient comfort were ensured with a combination of 6.0 PGA and 6.0 polypropylene sutures, followed by the application of a composite dressing over the palatal wound.
Instrumentation: Precision with Specialized Blades and Kits
Microblade selection was essential to achieving delicate and precise tunneling. The clinician utilized the Surgistar Nordland blade in conjunction with the Salvin Tunnel blade to facilitate minimal trauma dissection. The tunneling procedure was further supported by the use of the Kern Tunneling Kit (Salvin), a comprehensive set specifically designed to perform controlled and efficient subperiosteal tunneling.

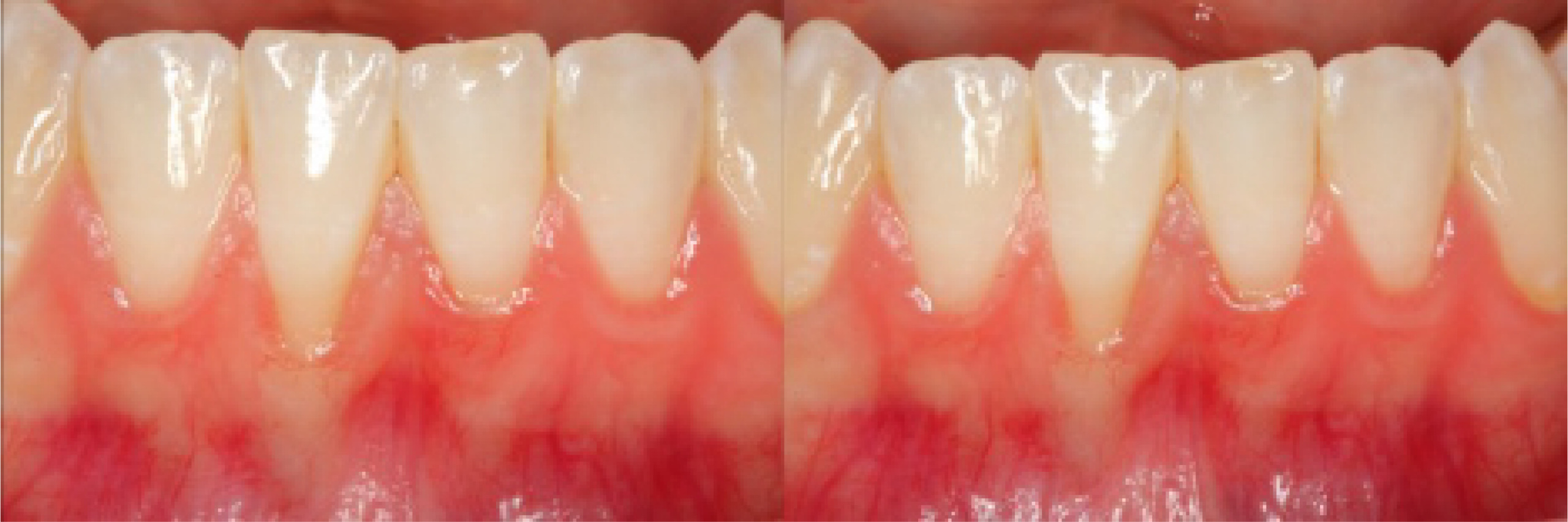
Healing and Outcomes
At 2 weeks post-operatively, the surgical site demonstrated healthy tissue adaptation, minimal inflammation, and stable graft integration. By 4 months, the treated area showed excellent tissue thickness, root coverage, and natural gingival contouring—indicative of successful soft tissue integration and vascularization.



Conclusion
Root coverage in the anterior mandible remains a demanding procedure, but with precise surgical techniques and the use of high-quality instrumentation and suturing methods, clinicians can achieve exceptional results. This case highlights the importance of case planning, anatomical respect, and surgical finesse in executing advanced soft tissue grafting procedures.
For clinicians looking to refine their skills in tunneling and connective tissue grafting, investing in hands-on training and staying updated with evolving techniques is key to clinical success.
Related CDOCS Hands-On Workshops
Hard and Soft Tissue Grafting in Digital Dental Implant Dentistry (CI250)
Deepen your implant expertise with hands-on training in bone and soft tissue grafting, flap management, socket grafting, sinus lifts, PRF technology, connective tissue harvesting, and complication prevention — building the surgical foundation for complex, predictable implant cases.

Advanced Hard and Soft Tissue Grafting in Digital Dental Implant Dentistry (CI260)
Master advanced bone and soft tissue grafting techniques, including socket grafting, autogenous connective tissue harvesting, transcrestal sinus lifts, staged ridge augmentation, and esthetic soft tissue grafting—all integrated with digital workflows and biological modifiers like PRF.