ENDODONTICS Article
Why Your Mandibular Block Keeps Failing on the Hot Tooth — and What to Do Instead
CDOCS Faculty
Dr. Louis Passauer, Jr.
CDOCS Faculty

The patient walks in holding a cup of ice water. Their lip goes numb after the block. You test, they feel it, and you give another. And another. The tooth is still hot.
If this has happened in your practice, the problem is not your technique on the individual injection. The problem is the protocol.
The hot mandibular molar is the most difficult tooth in the mouth to anesthetize. Irreversible pulpitis changes the tissue environment at a cellular level — the lowered pH around inflamed tissue blunts the effectiveness of standard lidocaine, and anaerobic bacteria in the pulp chamber produce gases that expand as the tooth returns to body temperature. The pain is real, the chemistry is working against you, and repeating the same inferior alveolar nerve block is one of the least effective ways to solve it.
Here is a protocol that works.
Start Before They Sit Down
Pre-medication changes the outcome before the patient opens their mouth. Ask patients with suspected irreversible pulpitis to take 400 mg of ibuprofen one hour before their appointment. Research published in the Journal of Endodontics in 2018 shows this meaningfully increases the success rate of pulpal anesthesia. It is a simple instruction that takes two seconds to relay and consistently improves what happens in the chair.
The Two-Block Protocol
Most dentists use a single IAN block and add more of the same if it fails. The more reliable approach is to combine two different blocks targeting different branches of the nerve.
Give one full carpule via the Gow-Gates mandibular nerve block. Then, while the patient holds their mouth open — which is critical and should be maintained for about two minutes — reload and give one full carpule via the standard IAN.
The timing works in your favor here. The two minutes the patient holds open to allow the Gow-Gates to settle is approximately the time it takes to reload and administer a slow IAN. Slow means 60 seconds per carpule, not 15. A study in the Journal of Endodontics from 2006 demonstrated that a slower injection rate produces a higher success rate of pulpal anesthesia — and a more comfortable one.
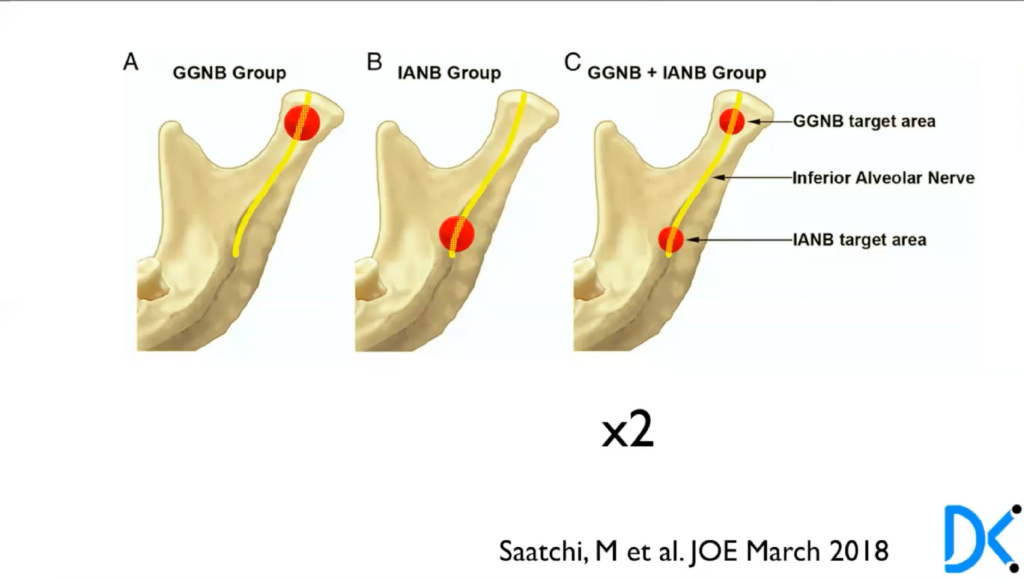
Research comparing the two-block combination against either technique alone shows nearly double the success rate for achieving pulpal anesthesia on the hot mandibular molar. That is not a marginal improvement. It is a protocol change worth making permanent.
Always Test Before You Start
A numb lip is not the same as pulpal anesthesia. Test with Endo Ice before picking up an instrument. If the patient responds to cold, do not give another mandibular block. Move to supplemental injections instead.
The sequence: start with an intraligamentary injection, test again, and proceed if there is no cold response. If still needed, move to an intraosseous injection — a Stabident or X-tip will deliver anesthetic directly into the bone adjacent to the tooth. Test again. If required, intrapulpal anesthesia is the last option: use a short needle with the bevel removed, advance into the canal until resistance is met, and administer with back pressure. It is not comfortable, but it works immediately.
One Protocol, Repeatable Results
The goal is a patient who feels no sensation to cold before you begin. Not a patient who says their lip is numb, not a patient who says it feels a little better — a patient who feels nothing when you apply cold to that tooth.
When that happens consistently, the clinical experience changes. The patient is calm. You are not managing pain during access. The procedure goes the way a root canal is supposed to go. And that patient, who walked in dreading the appointment, leaves having had a completely different experience than they expected.


One Protocol, Repeatable Results
Getting the hot mandibular molar numb is not about working harder on the injection you already know. It is about using the right combination: pre-medication an hour before, Gow-Gates plus IAN with a slow delivery, always testing before you start, and having a clear supplemental sequence ready when you need it.
Related CDOCS Hands-On Workshops
The General Dentist’s Playbook for Predictable Endodontic Therapy (CE110)
Build a complete, step-by-step endodontic skill set with hands-on training in case diagnosis, anesthesia, access cavities, glide path creation, canal shaping, irrigation, obturation, and coronal restoration.
Treating Complex Endodontic Cases with Confidence (CE210)
Advanced hands-on training in CBCT application, complex access cavities, challenging anatomy, reciprocation and rotary techniques, multiple obturation methods, and error recognition — tackling the cases most general dentists find hardest to treat.