 Mike Skramstad
Mike Skramstad It's not too often these days where I completely inherit and implant case. When I do, it's generally just a posterior implant that the patient has not restored yet for some reason. This one was a bit different. Was an implant placed on #8 and a crown on #9... ouch ;)
History:
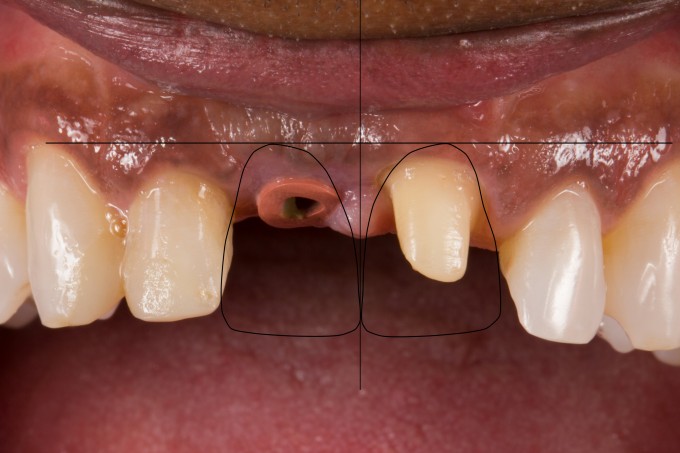
The patient suffered a trauma at work a year and a half ago. He had to have endo on #7 and #9 and tooth #8 was extracted. I asked if the implant was placed immediately and he said no... the implant was placed by the periodontist after 6 months of healing. He moved into my area 2 months ago and found his way to the oral surgeon I work closely with on referral. He then was referred to me to restore the implant and tooth. For the last year or so, he has been wearing a provisional acrylic cantilever bridge that was not even temporarily cemented, but held into place with denture adhesive. Here is how he presented to my office (he took his own temp off):

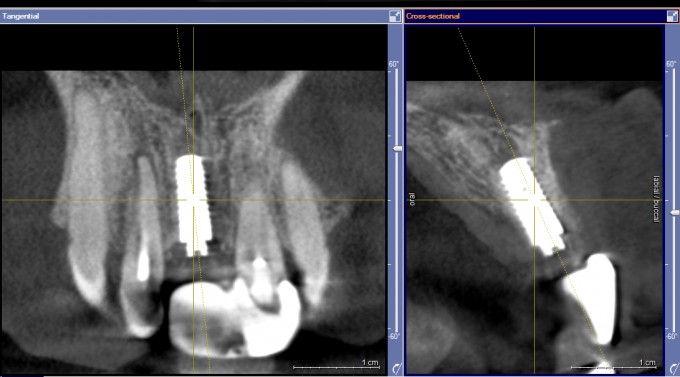
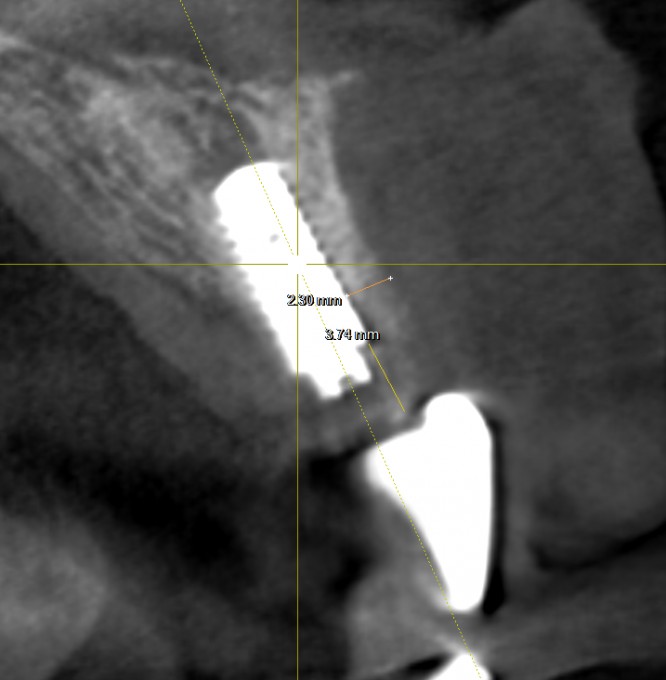
So, before I could even think about the restorative challenges on this case, I needed to take a 3D to evaluate where the implant was placed. Good news and good start because the Periodontist had excellent implant placement (Straumann BL 3.3)
Now I had to start thinking about the restorative challenges that we were facing. I could identify two right off the bat:
- The midline papilla was mostly lost and blunted. He did have a little on the lingual that I could play with, but I knew right away that I was going to have a long midline. It would have been nice if an immediate provisional was placed to hold the papilla right off the bat.
- The space was very asymmetric. That is, if I wanted the midline to be correct, the spaces were going to be far enough off that I would likely have to leave an open contact with tooth #10 to get proper proportions.
To verify my findings, I did a little planning before scanning the patient. Here are pictures of where I envisioned the midline, the asymmetric space, and where I planned the teeth to be:


So the next appointment we went ahead and scanned the patient for the restoration.
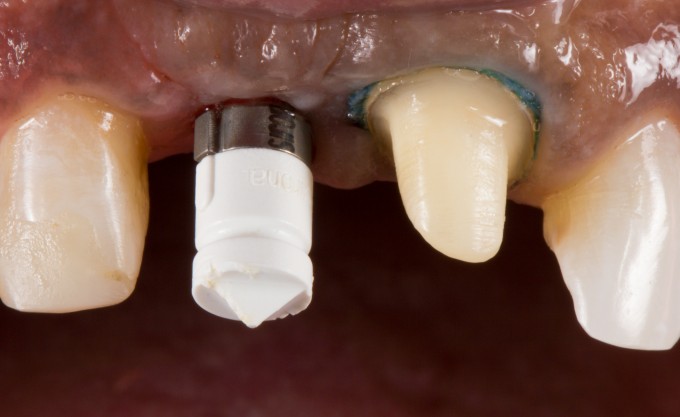
Designed the final restorations. I split #8 into a zirconia abutment and veneering structure. Both Crowns were e.max CAD V3 Impulse (had some left over before the introduction of MT)



Here was seat day yesterday:


The patient and I were both pretty happy with the final result... especially with how we started. After the first of the year we are going to reshape #10 and bond with composite and also restore #7 with a veneer to even out the color and shapes.
Now... 2 mistakes that I made on this case
- I made it very difficult from a color prospective milling an F.5 zirconia abutment (very white). I should have milled an F2 shade zirconia because it would have been profoundly easier to match the two teeth from a color prospective. The crowns were thin on the facial and #8 was clearly whiter than #9 due to the substrate underneath. I had to play around with resin cements (-3 value on #8 and +3 value on #9 were the final) to make this work. It was a pain in the neck.
- Since the implant was slightly lingual I had to create proper emergence on the facial by pushing on the tissue with the abutment. I over did it just a little bit and made the gingival crest slightly apical than where I would have wanted to be perfect. I did have a concavity there and maybe it will bounce back (this was immediate seat), but we will see. If not... no worries. Low lip line
Long story short... fun case , happy patient. Looking forward to finishing up the case next month